High Estrogen in Men: Causes, Symptoms & Management
High Estrogen in Men: Causes, Symptoms & Management
Most of the content online about high estrogen in men gets this backwards. It treats estradiol like a pure villain — something to crush, suppress, and eliminate. The reality is more complicated, and getting it wrong has real consequences. Estradiol is not optional for men. It drives libido, protects bone, and regulates fat distribution. Too much causes problems. Too little causes different — and sometimes worse — problems. Here's what the research actually shows.
The short answer: High estrogen in men — specifically elevated estradiol — can cause gynecomastia, low libido, erectile dysfunction, water retention, and mood changes. But estradiol is also essential for male bone health and sexual function. The goal is not to eliminate it. It is to keep it in the right range, identify the root cause, and address that root cause before reaching for medications that carry their own risks.
What Causes High Estrogen in Men?
High estrogen in men is almost always caused by excess aromatization — the enzymatic conversion of testosterone into estradiol. The four main drivers are obesity (the most modifiable), testosterone replacement therapy, liver disease, and certain medications. Estradiol in men comes almost entirely from this conversion process. Your body makes testosterone — in the testes, adrenals, and peripheral tissue — and an enzyme called aromatase converts a portion of it into estradiol. This is normal. The question is how much conversion is happening and where.
Obesity Is the Number One Modifiable Driver
Adipose tissue — body fat — is rich in aromatase. The more fat you carry, the more testosterone gets converted to estradiol. This is not a small effect. A 1980 study (Kley et al., 1980) found that in obese men, the conversion of androstenedione to estradiol correlated with ideal body weight at r = 0.82 — a strikingly strong relationship. As body fat increases, estradiol production rises and testosterone tends to fall, which is itself a cycle: low testosterone promotes fat gain, which promotes more aromatization, which further suppresses testosterone through estrogen-mediated negative feedback.
This mechanism explains why weight loss is often the most effective intervention for men with mildly elevated estradiol. The root cause — excess aromatase activity in fat tissue — gets addressed directly.
Testosterone Replacement Therapy
TRT introduces exogenous testosterone, which your body's aromatase then converts to estradiol. Higher circulating testosterone means more substrate for aromatization. Many men on TRT see their estradiol rise — sometimes substantially, especially at higher doses or with formulations that produce peak testosterone spikes (like weekly injections versus daily gel application). More frequent dosing reduces peak-to-trough variation and often results in more stable estradiol (Bhasin et al., 2018).
Liver Disease
The liver plays a central role in estrogen clearance. When liver function is impaired — from cirrhosis, alcoholic liver disease, or other causes — estradiol is cleared more slowly, allowing levels to accumulate. This is one reason gynecomastia is clinically associated with advanced liver disease (Braunstein, 1993).
Medications
Several drug classes interfere with sex hormone metabolism. Spironolactone (used for blood pressure and fluid retention) has anti-androgenic effects. Cimetidine (an older acid-suppressing medication) can elevate estradiol. Some antifungals — particularly ketoconazole — inhibit testosterone synthesis, altering the T-to-E2 ratio. If your estradiol has risen and you have started a new medication, that connection is worth reviewing with your provider.
Primary Hypogonadism and Genetic Conditions
Men with Klinefelter syndrome (XXY) typically have elevated gonadotropins and altered sex hormone profiles, often including elevated estradiol relative to testosterone. Some men also carry genetic aromatase variants that increase enzymatic activity, resulting in lifelong elevated conversion regardless of body composition.
What Are the Symptoms of High Estrogen in Men?
The symptoms of high estradiol in men overlap significantly with the symptoms of low testosterone — and the two conditions can coexist. Elevated estradiol through aromatization dysregulates feedback on the hypothalamic-pituitary axis, often suppressing LH and FSH secretion and thereby reducing testosterone production. So you can have symptoms from both at once.
Symptoms associated with significantly elevated estradiol in men include:
- Gynecomastia — true glandular breast tissue development, not simply chest fat. High estradiol stimulates breast gland proliferation. This is the most clinically specific sign of estrogen excess in men. See our article on gynecomastia in men for a full treatment breakdown.
- Low libido and erectile dysfunction — when estradiol is significantly out of ratio with testosterone, sexual function declines. The mechanism is partly direct and partly mediated through suppressed testosterone production.
- Water retention — estradiol has sodium-retaining effects via aldosterone pathways. Bloating and facial puffiness are commonly reported.
- Mood changes — emotional lability, irritability, and in some men, depressive symptoms have been reported with estradiol dysregulation in either direction.
These symptoms are non-specific. They are also the symptoms of low testosterone, poor sleep, obesity, thyroid dysfunction, and a dozen other conditions. Estradiol must be measured — not assumed — before attributing symptoms to it.
Estradiol in Men: What the Numbers Mean
| Range | Level (pg/mL) | Clinical Meaning |
|---|---|---|
How Is High Estrogen Diagnosed in Men?
The Assay Problem
Standard immunoassay estradiol tests are poorly validated for male estradiol levels — and almost nobody mentions this when ordering labs. The standard assay was designed for the female range — where estradiol runs 100-400 pg/mL across the cycle. In men, estradiol is typically in the 10-40 pg/mL range. At those low values, standard immunoassays have significant imprecision and cross-reactivity artifacts that can result in falsely elevated readings.
The clinical standard for accurate male estradiol measurement is liquid chromatography–tandem mass spectrometry — LC-MS/MS. A 2020 population study (Frederiksen et al., 2020) used LC-MS/MS to establish sex-specific reference intervals across the lifespan and found that adult men's estradiol typically runs 10-40 pg/mL (37-147 pmol/L) on an accurate assay. The distinction between assay types matters: an elevated estradiol result on a standard immunoassay should prompt confirmation with an LC-MS/MS assay before any treatment decision is made.
What "Normal" Looks Like
Reference ranges vary by lab and assay method. Using an LC-MS/MS assay, adult men's estradiol typically falls between 10 and 40 pg/mL (approximately 37-147 pmol/L). Levels below 10 pg/mL are associated with bone loss. Levels substantially above 40 pg/mL — particularly when accompanied by symptoms — are considered clinically elevated.
Context matters as much as the absolute number. A man on TRT with estradiol of 50 pg/mL and no symptoms may not need intervention. A man off TRT with the same number and gynecomastia probably does. The number alone does not dictate treatment.
Why Estradiol Is Essential for Men — Not Just "Too Much Is Bad"
Estradiol is biologically required for male bone health, libido, and sexual function — and suppressing it aggressively causes measurable harm. Two landmark randomized controlled trials from Massachusetts General Hospital established this with the clearest evidence available. Men are not supposed to have zero estradiol, and treatments that push it there carry real risks.
The 2013 NEJM RCT (Finkelstein et al., 2013) enrolled 198 healthy men, suppressed both testosterone and estradiol with goserelin and anastrozole, then randomized groups to receive varying testosterone doses with or without continued estradiol suppression. The results were unambiguous: sexual desire declined when testosterone was reduced — AND separately when estradiol was suppressed, even when testosterone levels were maintained. Both hormones are independently required for male libido.
The Bone Threshold: Why Under-Treatment Is Also Harmful
A 2016 follow-on study by the same group (Finkelstein et al., 2016) established a quantitative threshold: estradiol above 10 pg/mL and testosterone above 200 ng/dL were generally sufficient to prevent increases in bone resorption and decreases in bone mineral density in men. When estradiol dropped below that threshold — whether from disease or from medical suppression — bone resorption markers increased.
That 10 pg/mL floor is important when evaluating aromatase inhibitor therapy. Aggressive AI use that drives estradiol below that threshold is not neutral. It is harmful to bone.
Aromatase Deficiency in Men — The Natural Experiment
Before the Finkelstein RCTs, a case study from 1997 provided the earliest direct evidence of estradiol's role in men. Carani et al. (1997) described a man with a naturally occurring aromatase deficiency who had lifelong inability to convert testosterone to estradiol. His bone age was severely delayed, he had open epiphyses into adulthood, and he had markedly low bone density — despite normal testosterone. Estradiol replacement corrected these abnormalities. His body needed estradiol that his testosterone could not supply without aromatization.
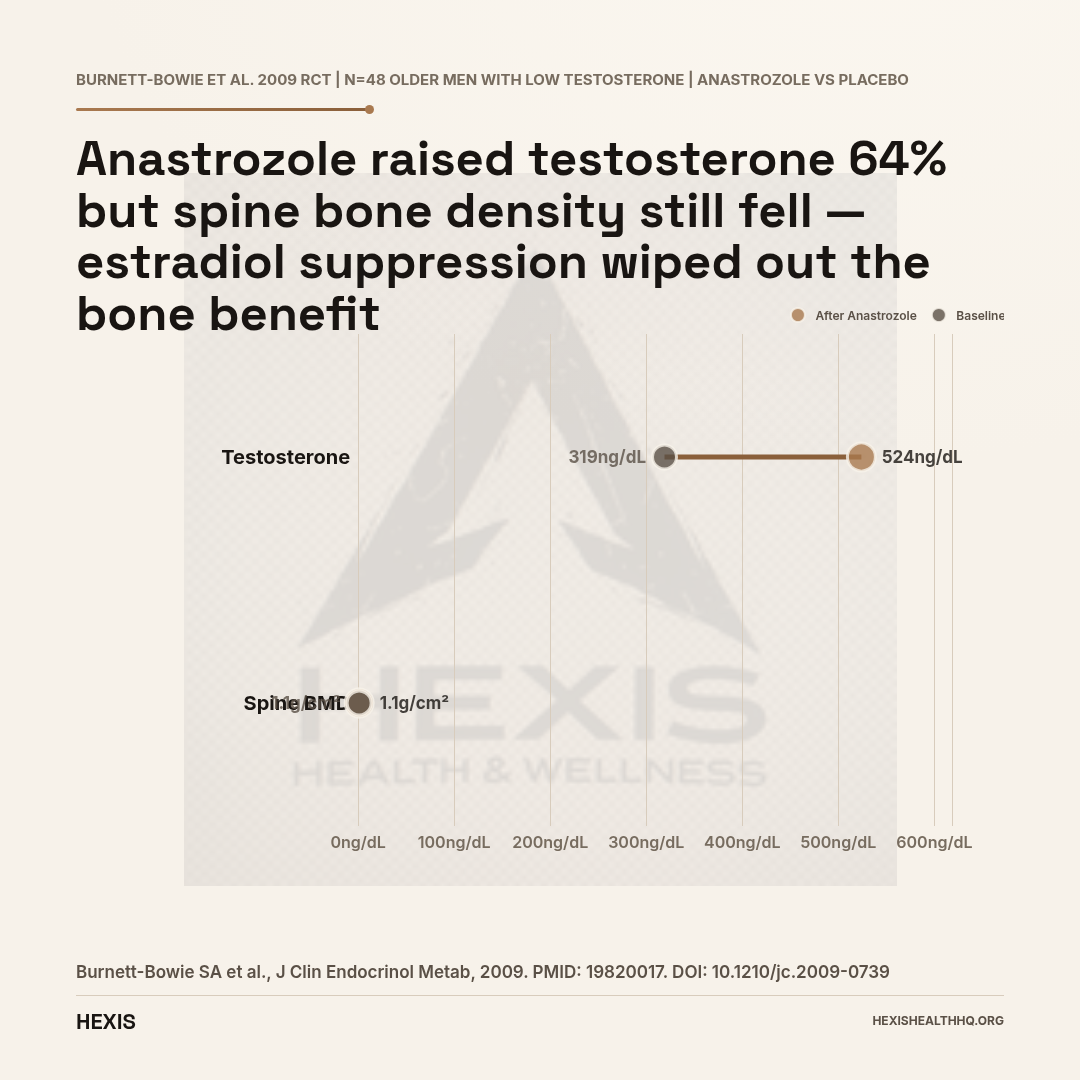
In a randomized controlled trial of older men with low testosterone, anastrozole reduced estradiol (15→12 pg/mL) and raised testosterone (319→524 ng/dL) — but posterior-anterior spine bone mineral density decreased compared to placebo (p = 0.0014). Estradiol suppression wiped out bone-protective effects before testosterone gains could compensate.
Source: Burnett-Bowie et al., J Clin Endocrinol Metab, 2009 (PMID 19820017)
The Aromatase Inhibitor Controversy: Should Men Use Anastrozole?
This is where the "lower estrogen = better" thinking causes the most harm.
Aromatase inhibitors — anastrozole (Arimidex) and letrozole — block the enzyme that converts testosterone to estradiol. They lower estradiol, raise testosterone (by removing estrogen's negative feedback on LH), and are frequently prescribed alongside TRT. But the evidence does not support routine AI use in men on TRT, and the Endocrine Society guidelines do not recommend it (Bhasin et al., 2018).
What the RCT Data Actually Show
Burnett-Bowie et al. (2009) ran a randomized controlled trial of anastrozole in older men with low testosterone. The drug did what it was supposed to — estradiol dropped (from approximately 15 to 12 pg/mL) and testosterone rose (from 319 to 524 ng/dL). But here is the finding that should give any prescribing clinician pause: posterior-anterior spine bone mineral density decreased in the anastrozole group compared to placebo (p = 0.0014). Testosterone went up. Estradiol went down past the protective threshold. Bones lost density.
Anastrozole raised testosterone and still caused bone loss — because the estradiol suppression wiped out estradiol's bone-protective effect faster than the testosterone gain could compensate. That's a result worth sitting with.
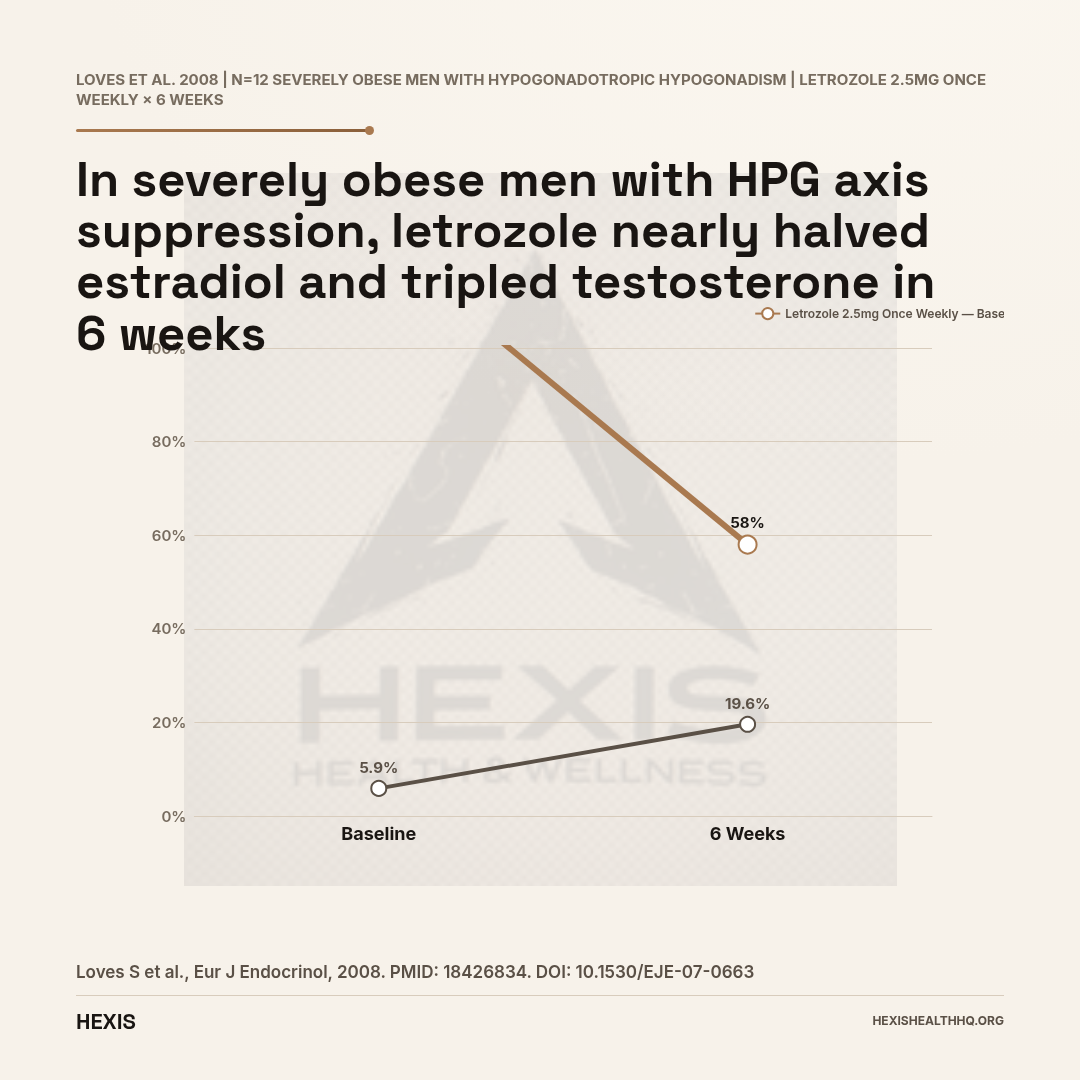
The data on letrozole in obese men tells a different story in a specific context. Loves et al. (2008) showed that letrozole once weekly significantly reduced estradiol (from 123 to 58 pmol/L) and raised testosterone (from 5.9 to 19.6 nmol/L, p<0.001) in severely obese men with hypogonadotropic hypogonadism. In that population — where massively elevated aromatase activity was suppressing the HPG axis — AI use addressed the root mechanism. That's a targeted case, not a template for routine TRT co-prescription.
When AIs Might Make Sense — and When They Don't
AIs are not appropriate for:
- Asymptomatic men with mildly elevated estradiol (no gynecomastia, no symptoms)
- Men on TRT who haven't yet tried dose or frequency adjustments
- Routine "estrogen management" without confirmed elevated levels on a sensitive assay
- Men who haven't addressed obesity as the underlying driver
AIs may have a role — under close supervision, with bone density monitoring — in:
- Men with confirmed, symptomatic estradiol elevation who have not responded to dose/frequency TRT adjustment
- Severely obese men with hypogonadotropic hypogonadism where aromatase activity is driving HPG axis suppression
- Specific cases of gynecomastia where other options have been exhausted
If you are on TRT and a provider is recommending anastrozole without first adjusting your injection frequency, dose, or delivery method, that conversation is worth having before filling the prescription. See our breakdown of TRT side effects and monitoring for more on what a reasonable monitoring protocol looks like.
How Is High Estrogen in Men Treated?
Treatment follows a three-step hierarchy: address the root cause first, adjust TRT dose or delivery method second, and consider aromatase inhibitors only as a last resort under clinical supervision. No number on a lab report automatically requires intervention — the clinical picture and symptoms drive the decision.
Step 1: Address the Root Cause
If obesity is driving aromatase activity — and in most men without TRT, it is — the primary intervention is weight loss. Not because it's the easy answer. Because reducing adipose tissue reduces aromatase activity, reduces estradiol production, and often raises testosterone through a combination of reduced negative feedback and improved HPG axis function. No medication needed. No side effects. No bone loss risk.
Similarly, if a medication is the culprit, changing or stopping it (where clinically appropriate) is the first move, not adding an aromatase inhibitor on top.
Step 2: Adjust TRT Dose and Frequency (If TRT-Related)
Men on injectable testosterone who are experiencing elevated estradiol have several levers before an AI. Dividing the same weekly dose into twice-weekly or more frequent injections reduces the peak testosterone concentration and therefore reduces peak aromatization. Switching delivery methods — from depot injection to daily gel — often results in lower and more stable estradiol without any medication change. For some men, a modest dose reduction is all that's needed.
This is why the Endocrine Society guidelines emphasize monitoring estradiol on TRT — not to preemptively suppress it, but to flag when it is rising in ways that correspond to symptoms that can't be explained by other causes (Bhasin et al., 2018).
Step 3: AIs as a Last Resort Under Supervision
If the above steps don't resolve symptomatic elevated estradiol, aromatase inhibitors can be considered — but not as a first-line move and not without monitoring. Bone density baseline before initiating AI therapy is reasonable. Periodic estradiol checks to confirm levels aren't being driven below the 10 pg/mL protective floor are essential. The goal is to bring estradiol into the appropriate range, not to eliminate it.
If you are considering this and want a provider who will actually look at your full picture — estradiol, testosterone, symptoms, body composition — rather than just reacting to a lab number, that is exactly how HEXIS approaches it. Schedule a consultation and we start with a full hormone panel, not a guess.
What About Injectable Testosterone and Estrogen?
There is no single estradiol target that applies to all men on injectable testosterone — the right level depends on symptoms, testosterone context, and injection frequency. Weekly depot injections create peak-to-trough variation in testosterone that drives corresponding estradiol variation. A man who injects 200 mg weekly will have very different estradiol dynamics than a man on 100 mg twice weekly — even at the same total weekly dose.
What matters is your estradiol in the context of your symptoms and your testosterone. A moderately elevated estradiol in a man who feels well, has good libido, and has no gynecomastia is not an emergency. A modestly elevated estradiol in a man with early gynecomastia and declining sexual function warrants attention. See our full breakdown of injectable testosterone protocols for more on how dosing decisions interact with estradiol management.
Frequently Asked Questions
What is a normal estradiol level for men?
Using a sensitive LC-MS/MS assay, normal estradiol in adult men is typically 10–40 pg/mL (37–147 pmol/L). Standard immunoassay tests are less accurate at male estradiol levels and can overestimate. If your result came back on a standard lab panel without specifying the assay type, ask your provider whether it was confirmed with LC-MS/MS — especially if a treatment decision is being made based on it (Frederiksen et al., 2020).
Should men on TRT take anastrozole?
Not routinely. The Endocrine Society does not recommend aromatase inhibitors as standard co-therapy with TRT. Anastrozole suppresses estradiol — which sounds like a win — but estradiol is essential for bone health in men. A clinical trial found that anastrozole caused spine bone density loss even while raising testosterone (Burnett-Bowie et al., 2009). Before adding an AI, dose and frequency adjustments to TRT should be tried first.
Can losing weight lower estrogen in men?
Yes, and it is the most evidence-based first-line intervention for obesity-related elevated estradiol. Fat tissue is the primary site of aromatase activity outside the gonads. Reducing body fat directly reduces aromatase-mediated testosterone-to-estradiol conversion (Kley et al., 1980). Many men who lose significant weight see their testosterone rise and estradiol normalize without any medication.
Does high estrogen cause gynecomastia in men?
Yes, estradiol excess relative to testosterone is the primary hormonal mechanism behind gynecomastia — the development of true glandular breast tissue in men. High estradiol stimulates breast gland proliferation. This is one of the most clinically specific signs of estrogen excess (Braunstein, 1993). For a detailed breakdown of causes, grades, and treatment options, see our article on gynecomastia in men.
Can high estrogen cause erectile dysfunction in men?
Yes, though the relationship is bidirectional and context-dependent. Severely elevated estradiol — particularly when paired with low testosterone — is associated with erectile dysfunction and low libido. But very low estradiol also impairs sexual function. The Finkelstein 2013 NEJM trial showed that estradiol suppression in men — independent of testosterone levels — reduced sexual desire. The goal is not low estradiol. It is appropriate estradiol in the right ratio with testosterone (Finkelstein et al., 2013).
The Bottom Line on High Estrogen in Men
High estrogen in men is real, it causes real symptoms, and it deserves real attention. But the treatment framework online — "estrogen is bad, take an AI" — is oversimplified to the point of being harmful.
Estradiol is essential for male bone health, libido, and sexual function. Aromatase inhibitors lower estradiol but carry bone loss risk when estradiol is pushed below the protective threshold. The evidence from randomized trials is unambiguous on this. Routine AI use alongside TRT is not evidence-based and is not recommended by the Endocrine Society.
Identify the root cause — obesity, TRT dose, medication, or underlying condition — address that first, and reserve aromatase inhibitors for cases where symptoms are confirmed, estradiol is accurately measured, and other options have been exhausted.
Your estradiol is not supposed to be zero. It is supposed to be in range.
The Bottom Line
- 1
Estradiol is essential for male bone health, libido, and sexual function — the goal is the right range, not zero.
- 2
Obesity is the #1 modifiable driver: fat tissue aromatase converts testosterone to estradiol at r=0.82 correlation.
- 3
Accurate diagnosis requires LC-MS/MS assay (not standard immunoassay) with reference range 10–40 pg/mL.
- 4
Anastrozole causes spine bone loss even while raising testosterone — routine AI use with TRT is not evidence-based.
- 5
Treatment hierarchy: weight loss → TRT dose/frequency adjustment → AI only as last resort with bone monitoring.