Injectable Testosterone: How TRT Injections Work
Injectable Testosterone: How TRT Injections Work
If you've been diagnosed with low testosterone and your doctor mentioned injections, you probably have questions nobody actually answered. How does it work? Which ester? How often? Does it hurt? What can go wrong? This is the breakdown — based on FDA labels, pharmacokinetic data, and the largest clinical trial on TRT ever run.
Injectable testosterone delivers the hormone into muscle or fat tissue, where it absorbs slowly into the bloodstream. FDA-approved for male hypogonadism, it requires a prescription and is a Schedule III controlled substance. Most protocols use testosterone cypionate or enanthate every 1–2 weeks, though many clinicians now dose more frequently to reduce hormonal peaks and troughs.
What Is Injectable Testosterone and Who Is It For?
Injectable testosterone is the delivery method, not the drug itself. The active hormone — testosterone — is the same regardless of how it gets into your body. Injections just happen to be the most reliable way to put it there.
The FDA has approved injectable testosterone for men with hypogonadism — a condition where the testes don't produce enough testosterone (Barbonetti, D'Andrea, and Francavilla, 2020). That diagnosis requires two morning serum testosterone readings below the lab reference range (most commonly below 300 ng/dL) plus documented symptoms: fatigue, low libido, loss of muscle mass, mood changes.
There are two types of hypogonadism. Primary hypogonadism means the problem is in the testes themselves — Klinefelter syndrome is one example (Kanakis and Nieschlag, 2018). Secondary (hypogonadotropic) hypogonadism means the signal from the brain — LH and FSH — is inadequate, so the testes don't get the cue to produce. Both are indications for TRT (Ide, Vanderschueren, and Antonio, 2020).
A lot of men in their 40s and 50s experience declining testosterone without a clear diagnosable cause. This is called late-onset hypogonadism, and it sits in a gray zone — symptoms are real, labs may be borderline, and treatment decisions require a conversation with a provider who understands both sides of the equation (Foresta et al., 2015). Testosterone levels should be measured on two separate morning draws before any diagnosis is confirmed — a single afternoon reading can miss the mark by 30% or more (Livingston et al., 2017).
Injectable testosterone is not approved for athletic performance enhancement or bodybuilding. It is a Schedule III controlled substance in the United States — legally available only with a physician's prescription.
The Three Injectable Esters: Cypionate, Enanthate, and Undecanoate
The "ester" is the key to understanding why different injectable testosterones behave differently. Testosterone itself is attached to a fatty acid chain (the ester) to slow its release after injection. Longer chain = slower release = less frequent dosing needed.
Testosterone Cypionate (Depo-Testosterone)
Testosterone cypionate is the most commonly prescribed injectable in the US. The standard formulation is 200 mg/mL in cottonseed oil. Per the FDA label, the half-life of testosterone cypionate when injected intramuscularly is approximately eight days.
That eight-day half-life means testosterone cypionate peaks within 24–72 hours after injection and then slowly declines. On a standard every-two-week protocol, testosterone levels can swing dramatically — high near injection day, low by day 14. Many clinicians now split the dose and inject every 5–7 days intramuscularly (or every 2–4 days subcutaneously) to keep levels more stable. The FDA label indicates dosing intervals of two to four weeks, but clinical practice has moved toward higher frequency in most TRT-focused clinics.
Testosterone Enanthate
Testosterone enanthate is the other workhorse of injectable TRT. It's essentially interchangeable with cypionate in practice — very similar half-life, similar peak-trough behavior, same dosing frequency range. The main difference is the carrier oil (sesame vs. cottonseed) and the fact that enanthate is more commonly used in research studies worldwide.
Xyosted is the FDA-approved subcutaneous enanthate formulation (NDA 209082). It's designed specifically for self-injection into the abdomen. More on subcutaneous injections in a moment.
Testosterone Undecanoate (Aveed)
Testosterone undecanoate is a different animal. Aveed (NDA 202763) is dosed at 750 mg/3 mL intramuscularly and is given according to a specific schedule: a loading dose, another dose at four weeks, then every ten weeks after that. The dramatically longer dosing interval comes from the much longer ester chain.
Aveed requires a REMS (Risk Evaluation and Mitigation Strategy) program. This is not a minor bureaucratic note — it's a hard regulatory requirement. The reason: pulmonary oil microembolism (POME) and serious anaphylaxis have occurred post-injection. Aveed must be administered in a certified healthcare setting by a trained provider. Patients must be observed for 30 minutes after each injection. This is not a home self-inject option.
If your goal is a convenient home-injection protocol, Aveed is not it. Cypionate and enanthate are the practical options for most patients.
Aveed Requires a REMS Program — It Is Not a Home-Inject Option
Testosterone undecanoate (Aveed, 750 mg/3 mL IM) carries mandatory FDA REMS requirements due to pulmonary oil microembolism (POME) and anaphylaxis risk. It must be administered in a certified healthcare setting. Patients must be observed for 30 minutes after each injection.
Source: FDA REMS — NDA 202763
How Testosterone Cypionate Works in Your Body: The Pharmacokinetics
Testosterone cypionate is absorbed from an oil depot at the injection site, with the ester cleaved in the bloodstream to release active testosterone. The pharmacokinetics determine why dosing frequency matters as much as dose amount.
Testosterone in plasma is 98 percent bound to a specific testosterone-estradiol binding globulin (SHBG), with about 2 percent free. That free fraction is the biologically active portion — the testosterone that actually does anything at the cellular level. This is why SHBG levels matter: two men with the same total testosterone can have very different amounts of free, active hormone depending on their SHBG.
Testosterone cypionate is metabolized primarily in the liver. About 90 percent of a dose is excreted in the urine as glucuronic and sulfuric acid conjugates, and about 6 percent of a dose is excreted in the feces, mostly in the unconjugated form.
The eight-day half-life means: inject 100 mg on Day 1, and you'll still have ~50 mg equivalent circulating on Day 8, ~25 mg on Day 16, and so on. This is why twice-weekly injections (splitting a typical 100–200 mg weekly dose into two equal injections) maintain far more stable trough levels than a single weekly injection.
Testosterone also converts (aromatizes) to estradiol. This is normal and necessary — estradiol plays real roles in bone health, mood, and cardiovascular function in men. But at higher testosterone levels, some men convert enough that estradiol rises into a range that causes gynecomastia (breast tissue development) or water retention. Some providers add an aromatase inhibitor (AI) to manage this; others monitor and adjust dose instead. This is one of many reasons why TRT requires ongoing lab monitoring, not just an initial prescription.
IM vs. Subcutaneous: Which Route Is Better?
Intramuscular (IM) injection means the needle goes into muscle tissue — typically the glute (ventrogluteal or dorsogluteal site), the vastus lateralis (outer thigh), or the deltoid. Standard IM needles are 1–1.5 inches, 22–25 gauge.
Subcutaneous (SC) injection means the needle goes into the fat layer just beneath the skin — the abdomen or outer thigh are common sites. SC needles are shorter and finer, usually 5/8 inch, 25–27 gauge.
The pharmacokinetic difference matters. IM injections produce higher peak levels and faster absorption. SC injections produce a slower, flatter absorption curve — lower peaks, higher troughs, less overall swing. For men who feel the hormonal peaks and valleys on standard IM dosing, SC injections can smooth the ride. They're also easier to self-administer for many people since the injection depth is shallower and pain tends to be less.
The evidence base for SC testosterone injection is growing but still thinner than for IM (Tsametis and Isidori, 2018). Most FDA label data and long-term safety studies are based on IM administration. Both routes are used clinically, and neither has been proven definitively superior in head-to-head outcomes data. The choice depends on patient preference, body composition, and how well the patient tolerates the peak-trough cycle.
IM vs. Subcutaneous Injection — Key Differences
| Feature | Intramuscular (IM) | Subcutaneous (SC) |
|---|---|---|
Source: FDA label; Tsametis and Isidori, 2018
What Does the Research Actually Show? The TRAVERSE Trial
The largest and most important piece of evidence on TRT safety in recent years is the TRAVERSE trial (NCT03518034). Among 5,204 men aged 45–80 with hypogonadism and established or high cardiovascular risk, testosterone replacement therapy was compared to placebo over a median follow-up period (Pencina et al., 2024).
That trial answered one of the biggest questions hanging over TRT for years: does it increase heart attack or stroke risk? The answer was no — TRT was noninferior to placebo for major adverse cardiovascular events (MACE). The prior FDA black-box cardiovascular concern had driven many physicians away from prescribing TRT; TRAVERSE substantially changed that calculus.
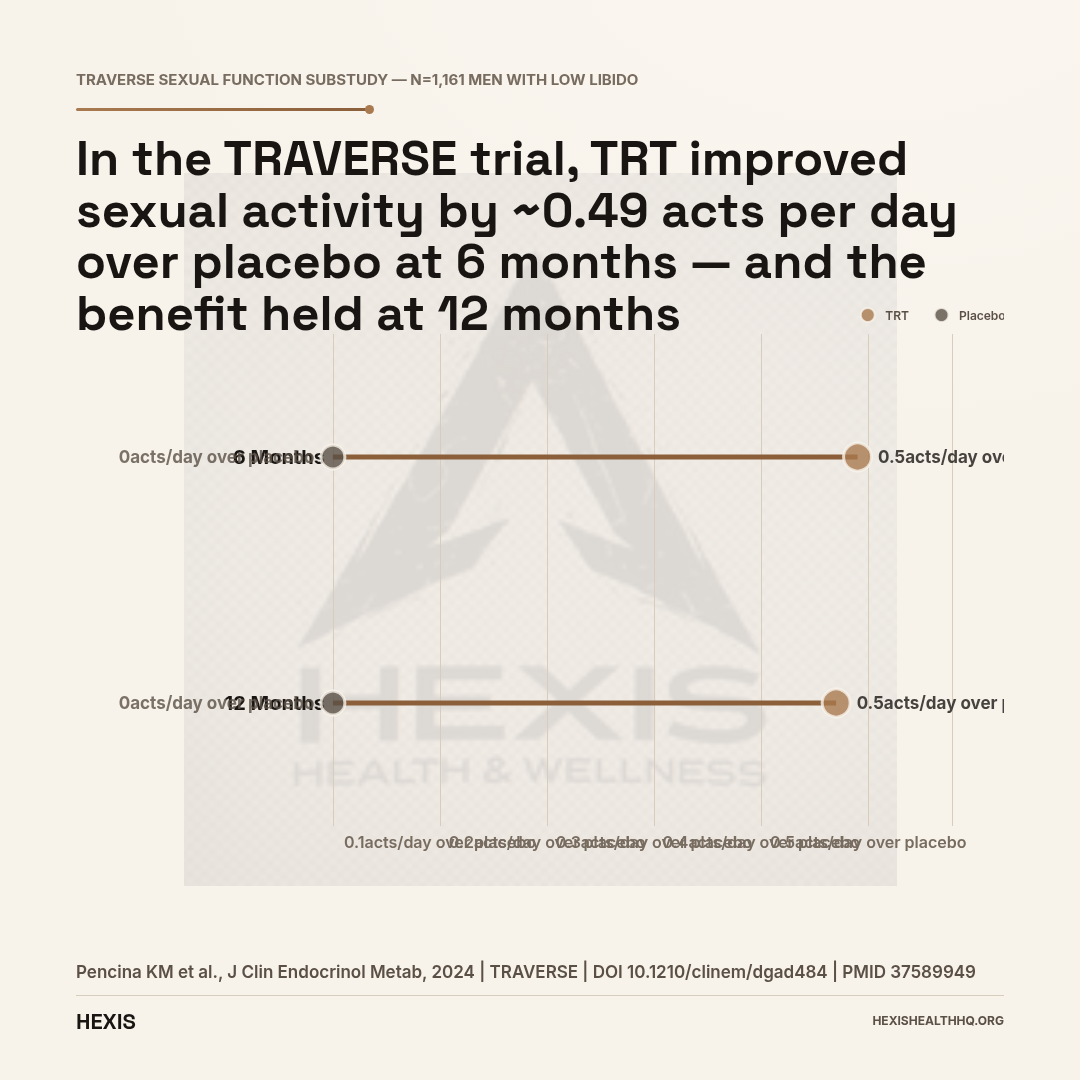
The TRAVERSE sexual function substudy enrolled 1,161 men with low libido (Pencina et al., 2024). The TRT arm showed a mean improvement in sexual activity of 0.49 acts per day over placebo at 6 months (95% CI [0.19, 0.79]) and 0.47 acts per day at 12 months (95% CI [0.11, 0.83]). That's a statistically significant improvement in a real, measured clinical outcome. Worth knowing if you're wondering whether TRT actually works for the most common complaint.
Prostate Safety
Before TRAVERSE, physicians were cautious about TRT and prostate cancer. The TRAVERSE prostate substudy (Bhasin et al., 2023) enrolled over 5,000 men and found no significant increase in high-grade prostate cancer with TRT versus placebo (PMID 38150256). This was a randomized clinical trial, not observational data — the strongest type of evidence. The trial did find that prostate-specific antigen (PSA) rose modestly with TRT, so ongoing monitoring remains important, but the feared connection to high-grade prostate cancer was not supported.
Depression and Mood
Depressive syndromes improved significantly in hypogonadal men who received TRT in the TRAVERSE depression substudy (Bhasin et al., 2024, PMID 38205962). This is consistent with the well-documented relationship between testosterone and mood regulation — testosterone affects dopaminergic and serotonergic signaling pathways in ways that are relevant to depression and motivation, not just libido.
Side Effects Worth Knowing About
TRT's side effects are real, dose-dependent, and manageable with monitoring. None of these are reasons to avoid the therapy — but all of them are reasons why monitoring matters.
Hematocrit Elevation (Polycythemia)
This is the most clinically significant dose-dependent side effect. Testosterone stimulates red blood cell production. If hematocrit rises too high — above 54% is the commonly used threshold — blood thickens, increasing clot risk. This is why hematocrit monitoring is a non-negotiable part of TRT management.
Dose reduction or phlebotomy (blood donation or therapeutic phlebotomy) are the management options. Some men on TRT have used blood donation as a management strategy, though eligibility rules vary and FDA guidelines for donation from TRT patients require careful interpretation (Chin-Yee et al., 2017).
Estradiol Rise and Gynecomastia
Testosterone aromatizes to estradiol at varying rates from person to person. Nipple tenderness or breast tissue development signals that estradiol has climbed into a problematic range. This is manageable — usually with dose adjustment, sometimes with an aromatase inhibitor.
Injection Site Pain
Post-injection pain and bruising are common, especially with IM injections into the glute or quad. Warming the oil to body temperature before injection reduces pain. Injecting slowly (over 30–60 seconds rather than 5), rotating sites, and using smaller gauge needles all help. Most people adapt within the first few weeks.
Suppression of Natural Testosterone Production and Fertility
Exogenous testosterone suppresses the hypothalamic-pituitary-gonadal (HPG) axis. Your brain reduces LH and FSH output because it senses circulating testosterone is adequate. The testes get less stimulation and shrink somewhat. Natural testosterone production falls, often to zero. Sperm production is severely reduced — this is a near-universal effect and should be discussed before starting TRT if fertility is a current concern (Rastrelli et al., 2019).
Human chorionic gonadotropin (HCG) can be added to TRT protocols to maintain testicular stimulation and preserve some fertility. This is a separate conversation with your provider — not a DIY decision. See our overview of HCG and TRT protocols for how that combination works in practice.
FAERS Data in Context
The FDA's adverse event reporting system (FAERS) contains 51,926 adverse event reports on file for testosterone across all formulations. That number sounds alarming. It isn't — without context. FAERS is passive surveillance: reports filed voluntarily, no causation established. Someone experiencing something while taking the drug gets logged; that doesn't mean the drug caused it. Most serious events in FAERS overlap with the known side effect profile: cardiovascular events, hematocrit elevation, injection site reactions. The data shapes monitoring protocols. It does not condemn the therapy.
Hematocrit Above 54% Requires Intervention
Testosterone stimulates red blood cell production. If hematocrit exceeds 54%, blood thickens and clot risk rises. This is the most clinically significant dose-dependent side effect of TRT. Routine monitoring is required — hematocrit is checked at baseline and at follow-up labs. Management: dose reduction or phlebotomy.
Source: Chin-Yee et al., Transfusion, 2017 — PMID 28150363
Injectable Testosterone vs. Testosterone Gels
Injectable testosterone and topical gels both deliver the same hormone — the differences are compliance burden, transfer risk, cost, and how stable your levels stay between doses. For most patients without a needle contraindication, injections offer better pharmacokinetic control at significantly lower cost.
Gels (like AndroGel) are applied daily to skin — usually shoulders or upper arms. They produce relatively stable serum levels without the peak-trough cycle. The catch: they carry a real skin-transfer risk. Partners and children who come into contact with gel-treated skin before it dries can absorb testosterone. This is a documented problem, not a theoretical one. Gels require daily compliance, and forgetting a day noticeably affects levels.
Injections bypass the transfer problem entirely. You inject once a week (or more often with smaller doses), no daily compliance burden, and no contamination risk to others. Cost-wise, injectable testosterone is significantly cheaper — generic testosterone cypionate is one of the most affordable TRT options available. The downside is that needles require a technique learning curve, and the peak-trough cycle can cause some men to feel the hormonal swing.
Most patients who understand both options and have no needle aversion prefer injections. The pharmacokinetic control — especially with more frequent dosing — is simply better.
Athletic Eligibility: WADA and TUE
If you compete in any sport governed by the World Anti-Doping Agency (WADA), this section matters.
Testosterone is classified as a WADA S1 Anabolic Agent (Anabolic Androgenic Steroid). It is prohibited at all times — both in-competition and out-of-competition. There are no level thresholds that make it permissible without a Therapeutic Use Exemption (TUE).
A TUE is available for athletes with documented hypogonadism — the diagnosis must be confirmed with appropriate lab work, clinical documentation, and submitted for review. The TUE process takes time and has specific requirements. If you're a competitive athlete considering TRT, start that TUE application before beginning therapy, not after.
USADA (the US Anti-Doping Agency) follows WADA's prohibited list. So do essentially all international sport governing bodies. "But my doctor prescribed it" is not a defense without a valid TUE on file.
How to Inject Testosterone: The Practical Reality
A standard intramuscular testosterone injection uses an 18-gauge draw needle to fill the syringe, then a 22–25 gauge, 1–1.5 inch needle for the actual injection — delivered at a 90-degree angle into muscle, slowly over 30–60 seconds. You'll be trained by your provider or their staff before your first self-injection. The general sequence for an IM injection into the glute looks like this:
Wash your hands. Draw the dose through a larger drawing needle (18-gauge is common), then swap to the injection needle (22-25 gauge, 1–1.5 inch depending on body composition). Wipe the injection site with an alcohol swab and let it dry. Insert the needle at a 90-degree angle with a smooth, confident motion — hesitation causes more pain, not less. Inject slowly — 30 to 60 seconds for 1 mL. Remove and apply gentle pressure.
Rotate your injection sites. Hitting the same spot repeatedly causes scar tissue buildup (lipohypertrophy), which impairs absorption over time. Alternating glutes (or quad, or ventrogluteal) keeps absorption consistent.
Subcutaneous injections into the abdomen follow the same preparation steps with a shorter needle and a pinch-up technique on the fat tissue — far less intimidating for most people new to injections.
What to Expect on TRT: Timeline
Most men on TRT notice mood and libido improvements within 2–4 weeks, with energy and body composition changes becoming apparent by weeks 4–8. Full symptom response — confirmed by stabilized lab levels — typically takes 3–6 months, consistent with TRAVERSE trial data (Pencina et al., 2024). Testosterone doesn't transform you overnight, but the timeline is predictable:
- Weeks 1–3: Improved sleep, libido may begin improving, mood often the first to shift
- Weeks 4–8: Energy improvements more noticeable, some lean mass gains beginning
- Month 3–6: Lab levels stabilize, body composition changes become measurable, TRAVERSE data shows sexual function improvements by 6 months (Pencina et al., 2024)
- Month 6+: Full symptom response typically established; ongoing monitoring for hematocrit, PSA, and estradiol becomes routine
Protocol adjustments are common in the first six months. Your lab draw should occur at trough (the day before or morning of your next injection) for the most clinically meaningful comparison across time points. Age also factors into expectations — testosterone's effects on muscle mass and vitality are well-documented in older men, but the magnitude of response varies with baseline levels and how long deficiency has been present (Barone et al., 2022).
Frequently Asked Questions About TRT Injections
How often do you inject testosterone cypionate?
The FDA label for testosterone cypionate specifies dosing intervals of two to four weeks. In clinical practice, most TRT-focused providers dose it every seven days (weekly) or twice weekly to reduce the peak-trough swing that comes with longer intervals. Some patients inject every 3–4 days subcutaneously for the flattest possible curve.
Can I do subcutaneous testosterone injections at home?
Yes — subcutaneous testosterone injection is a legitimate route practiced by many patients on home-based TRT protocols. The technique is shallower and generally less painful than IM. Your provider needs to prescribe the appropriate concentration and needle size for SC use.
Will testosterone injections affect my fertility?
Testosterone therapy suppresses sperm production in virtually all men who use it. This effect is typically reversible after discontinuation, but recovery time varies from months to over a year. If you want to preserve fertility, discuss HCG co-therapy or sperm banking before starting TRT (Rastrelli et al., 2019).
Is injectable testosterone safer than gels?
"Safer" depends on what risk you're measuring. Injections eliminate the skin-transfer risk of gels. Gels eliminate injection site complications. The TRAVERSE trial's cardiovascular safety data applies broadly to TRT — not specifically to one delivery method (Pencina et al., 2024). Both are FDA-approved; the choice involves practical factors more than a clear safety hierarchy.
Does TRT cause prostate cancer?
The TRAVERSE prostate substudy — a randomized controlled trial of over 5,000 men — found no significant increase in high-grade prostate cancer with testosterone replacement therapy compared to placebo (Bhasin et al., 2023). PSA monitoring is still required. Men with active prostate cancer are not candidates for TRT.
Starting TRT at HEXIS Health
HEXIS starts every TRT protocol with bloodwork. Not a questionnaire — actual labs. We look at total and free testosterone, LH, FSH, estradiol, complete blood count (for hematocrit baseline), PSA, and a metabolic panel. That baseline tells us where you're starting and what your protocol should look like. In practice, most patients we work with transition from a standard biweekly injection schedule to weekly dosing within the first one to two months — the difference in how they feel is almost always noticeable.
If injectable testosterone is the right fit, we build the protocol around your numbers — which ester, what dose, what frequency — not a template. Follow-up labs at six to eight weeks let us dial in the dose before locking in a long-term protocol. Ongoing monitoring covers the side effects that matter: hematocrit, estradiol, PSA.
If you want to understand what your numbers actually mean and whether TRT makes sense for you, Schedule a consultation. We don't prescribe without bloodwork. That's not a policy — that's medicine.
For more on how testosterone therapy fits into broader hormone optimization, see our overview of testosterone replacement therapy and what low testosterone symptoms actually feel like before you assume you need treatment. If you're also considering other delivery methods, our guide on testosterone gels vs injections breaks down the tradeoffs in more detail.
- 1
Injectable testosterone (cypionate, enanthate) is FDA-approved for male hypogonadism — diagnosis requires two low morning labs plus symptoms, not just a number.
- 2
The ~8-day half-life of cypionate means dosing frequency matters: every 5–7 days IM (or every 2–4 days SC) keeps levels more stable than the standard biweekly label dosing.
- 3
TRAVERSE (n=5,204) confirmed TRT is noninferior to placebo for cardiovascular events and showed no increase in high-grade prostate cancer — the two biggest historical concerns.
- 4
Hematocrit elevation is the most important dose-dependent side effect. It requires monitoring, not fear.
- 5
Aveed (undecanoate) requires REMS in-office administration — not a home protocol. Competing athletes need a TUE before starting any TRT.