HRT Side Effects in Women: What the Evidence Actually Says
HRT Side Effects in Women: What the Evidence Actually Says
If you stopped HRT after reading the 2002 Women's Health Initiative headlines — or if you're afraid to start because of what you've heard about breast cancer and blood clots — this article is for you. At HEXIS, these are the conversations our physicians have most often with perimenopausal and postmenopausal women: the science on HRT side effects in women is more nuanced than the scary headlines suggested, and most women deserve the actual numbers — not just relative risks that sound terrifying without context.
The short answer: HRT does carry real risks — breast cancer, blood clots, stroke — but for most healthy women starting before age 60 or within 10 years of menopause, those absolute risks are small, formulation matters enormously, and the risks look very different depending on whether you're taking a pill or a patch. Here's what the evidence actually shows.
Common Side Effects When You First Start HRT
Most women starting HRT experience a cluster of early side effects — breast tenderness, spotting, bloating, mood shifts — that resolve within two to three months and do not require stopping treatment.
Breast tenderness is among the most reported early complaints. It typically peaks in the first few weeks and eases with dose adjustment. Irregular bleeding or spotting is common with combined HRT, especially in the first few months, as the uterine lining adjusts. Women on cyclic regimens may experience withdrawal bleeds — this is expected. Persistent or unexpected bleeding always warrants evaluation, but early spotting alone is not cause for alarm.
Bloating and fluid retention can occur, particularly with oral estrogen, which has first-pass liver effects that transdermal routes bypass entirely (Arnautu et al., 2025). Mood changes — irritability, low mood, or mood swings — are reported by some women in the early adjustment phase, though the evidence is more reassuring than the reputation: multiple randomized trials show micronized progesterone does not cause depression and may actually improve sleep quality (Prior, 2018).
Headaches and nausea are more common with oral preparations and tend to be dose-dependent. If you're getting headaches on oral HRT, switching to a transdermal patch or gel is often enough to resolve them — the delivery route matters more than people realize.
None of that is fun. But early side effects are self-limiting in the vast majority of women — they are not the same as the serious long-term risks that require an actual risk-benefit analysis, and mixing them up is one reason women stop HRT prematurely.
What the WHI Study Actually Found — and What It Didn't
The 2002 Women's Health Initiative (WHI) trial is the source of most HRT fear — and most of that fear is based on a misunderstanding of what the study actually showed and who it studied.
The WHI enrolled 16,608 postmenopausal women and compared oral conjugated equine estrogen plus medroxyprogesterone acetate (CEE+MPA) against placebo over a mean of 5.2 years. The headline results showed increased risks for several outcomes (Rossouw et al., 2002):
- Breast cancer: hazard ratio 1.26 (95% CI 1.00–1.59)
- Stroke: HR 1.41 (95% CI 1.07–1.85)
- Pulmonary embolism: HR 2.13 (95% CI 1.39–3.25)
- Coronary heart disease: HR 1.29 (95% CI 1.02–1.63)
Those hazard ratios sound alarming. Here's what they look like in absolute terms, per 10,000 women per year:
- 8 additional breast cancers
- 8 additional strokes
- 8 additional pulmonary embolisms
- 7 additional CHD events
But also: 6 fewer colorectal cancers and 5 fewer hip fractures per 10,000 women per year (Rossouw et al., 2002).
That's 8 extra breast cancers per 10,000 women — not 26% of women getting breast cancer. The difference between the hazard ratio and the absolute risk is not a trick; it's the information you actually need to make a decision.
Critically: the average WHI participant was 63 years old — not the typical woman starting HRT at menopause onset around age 50. The trial used oral CEE+MPA, not transdermal estradiol with micronized progesterone. These distinctions are not minor footnotes; they fundamentally change the risk profile, as we'll cover below.
A 2026 reanalysis of the WHI data confirmed what has become known as the "timing hypothesis": for healthy women who start HRT before age 60 or within 10 years of menopause onset, the risk-benefit calculation looks very different than for older women or those with long post-menopausal gaps (Lambrinoudaki et al., 2026).
Does HRT Increase Breast Cancer Risk?
Breast cancer is the fear that stops most women from starting or continuing HRT. The honest answer is: it depends entirely on the formulation — and one specific component changes the picture more than anything else.
The WHI showed an increase in invasive breast cancer with combined CEE+MPA (Rossouw et al., 2002). But the WHI's estrogen-only arm — women who had already had a hysterectomy and took CEE without a progestogen — showed a marginal, non-significant reduction in breast cancer risk over seven years (Lambrinoudaki et al., 2026).
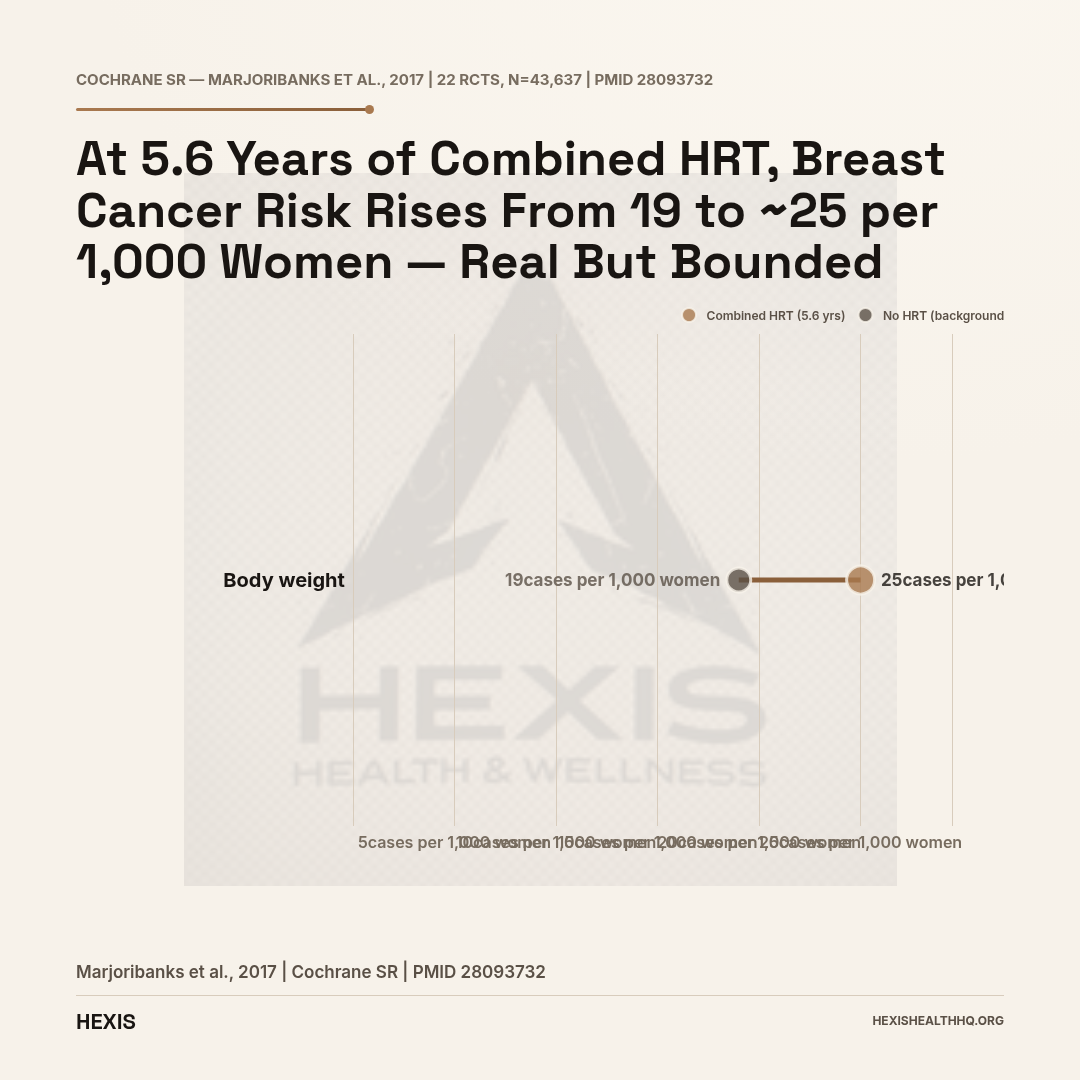
The Cochrane systematic review, which pooled 22 RCTs involving 43,637 women, put the absolute risk this way: at 5.6 years of combined HRT use, breast cancer incidence goes from roughly 19 per 1,000 women in the background population to 20–30 per 1,000 (Marjoribanks et al., 2017). That is a real increase — not imaginary — but it is also a small absolute increase over many years of treatment.
Progestogen type changes the breast cancer signal significantly. A narrative review of oncological outcomes found that progestins structurally related to testosterone (such as MPA, the progestin used in the WHI, and norethisterone) carry the highest breast cancer risk, with a relative risk of 3.35 (95% CI 1.07–10.4) compared to estrogen alone (D'Alonzo et al., 2019). By contrast, the large French E3N prospective cohort study — following more than 80,000 menopausal women over eight years — found that oral micronized progesterone used with estrogen did not increase breast cancer risk and may have been protective (Prior, 2018).
Most women — and many clinicians — don't know that MPA and micronized progesterone are treated as different drugs in the breast cancer evidence base. The standard MPA from the original WHI is not the same as Prometrium or Utrogestan, which is structurally identical to the progesterone your ovaries produced before menopause. That's not a marketing distinction. It changes the biology.
To put the breast cancer risk in context: the combined HRT breast cancer risk is roughly comparable to having one to two alcoholic drinks per day, and lower than the risk associated with obesity. That's not meant to minimize it — it's meant to put it in a frame that allows you to make a real decision.
Does HRT Cause Blood Clots?
Blood clots (venous thromboembolism, or VTE) are a real risk with HRT — but whether you're taking a pill or a patch makes a dramatic difference.
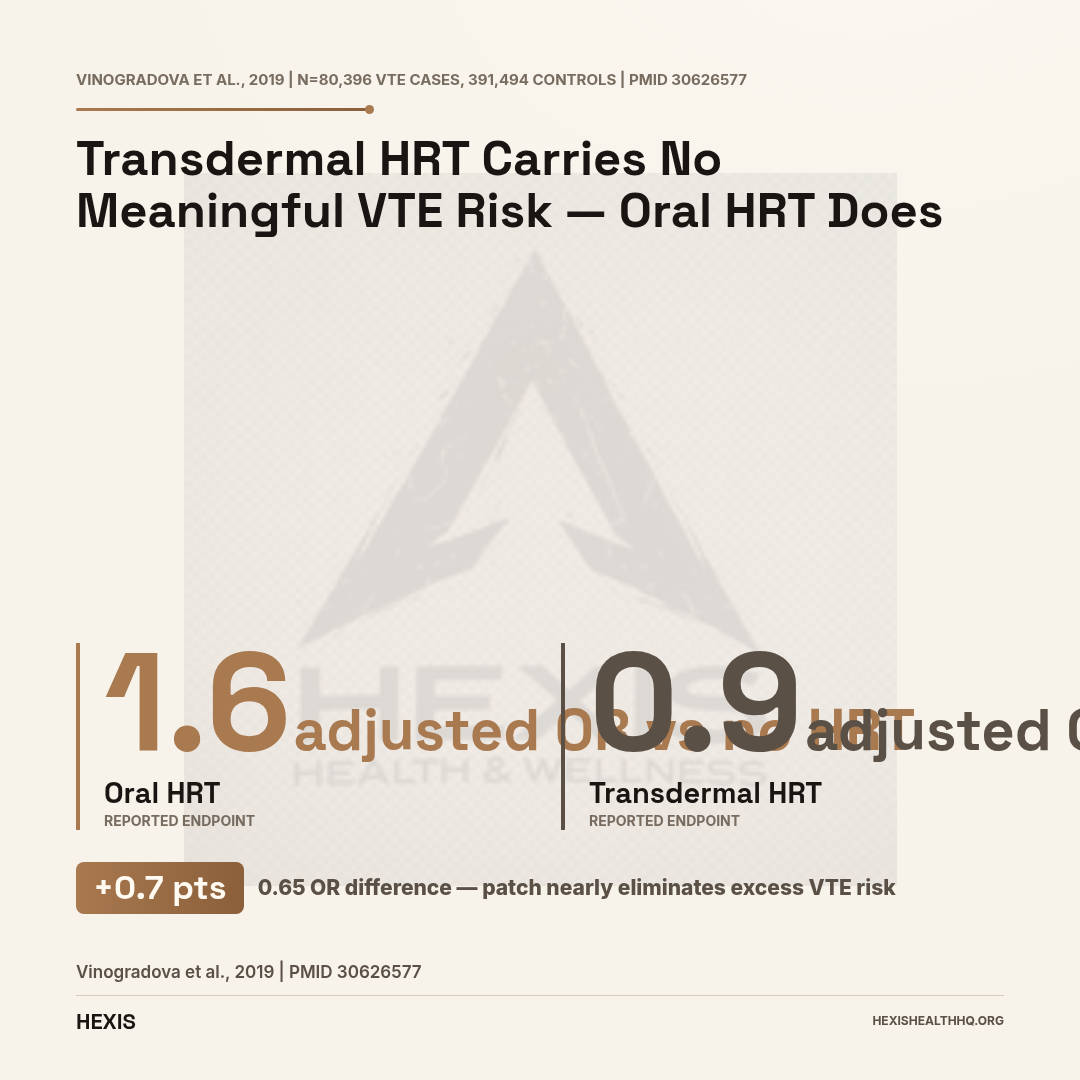
The largest study on this question looked at 80,396 women with VTE and 391,494 controls. Oral HRT was associated with a meaningful increase in VTE risk: adjusted OR 1.58 (95% CI 1.52–1.64). The highest-risk combination was oral CEE+MPA, with an OR of 2.10 (1.92–2.31). But transdermal preparations showed an adjusted OR of 0.93 (95% CI 0.87–1.01) — not significantly different from no HRT at all (Vinogradova et al., 2019).
This is not a marginal difference. It is the scientific basis for why most current UK and European guidelines recommend transdermal estradiol (patch, gel, spray) as the preferred route, especially for women with elevated VTE risk — such as those who smoke, have a higher BMI, or have a personal or family history of clots.
The Cochrane review's absolute numbers for VTE: in women under 60 taking combined HRT, the absolute risk of VTE is less than 1 in 500 per year (Marjoribanks et al., 2017). That's a small absolute risk for most women, but it is real and it's worth weighing — particularly if you have additional risk factors.
The mechanism behind the route difference is first-pass liver metabolism. Oral estrogen is processed by the liver on its way into circulation, which triggers clotting-factor changes. Transdermal estradiol bypasses the liver entirely, which is why it doesn't carry the same coagulation signal.
If you have any personal or family history of DVT, PE, or a clotting disorder, the transdermal route is not just preferable — it is the route supported by the evidence for women in your situation.
VTE Risk: Pill vs Patch
Adjusted odds ratio vs no HRT — Vinogradova et al., 2019 (BMJ, n=80,396 VTE cases)
| Route | Adjusted OR | vs No HRT |
|---|---|---|
| Oral HRT (all) | 1.58 | Significantly elevated |
| Oral CEE+MPA (highest risk) | 2.10 | Significantly elevated |
| Transdermal HRT (patch/gel/spray) | 0.93 | No significant increase |
Cardiovascular Risk: Why Timing Is Everything
HRT started before age 60 or within 10 years of menopause onset does not increase cardiovascular risk — and may reduce it. The cardiovascular harm seen in the WHI came from late initiation, not from HRT itself.
The WHI showed increased stroke and CHD risk overall — but the trial enrolled women with an average age of 63, many of whom were years past menopause. For these women, HRT was being initiated long after their cardiovascular window of opportunity had closed (Lambrinoudaki et al., 2026).
The timing hypothesis — now widely accepted across North American Menopause Society, International Menopause Society, and British Menopause Society guidelines — holds that HRT initiated before age 60 or within 10 years of menopause may confer cardiovascular benefit or neutrality, not harm. Delayed initiation, at 65 or more, is associated with increased coronary events and stroke (Lambrinoudaki et al., 2026).
What this means practically: a 50-year-old woman starting the patch at menopause has a very different cardiovascular risk profile than the 63-year-old average WHI participant. The WHI data does not apply directly to her situation — and acting as if it does has led to a generation of women suffering menopause symptoms unnecessarily.
For women navigating perimenopause symptoms, starting a conversation with a provider about timing is the most important factor in personalizing the risk-benefit analysis.
Endometrial Cancer Risk
This is one risk that is fully manageable — once you understand the rule.
Unopposed estrogen (estrogen without a progestogen) in women who still have a uterus significantly increases endometrial cancer risk. The FDA's Black Box Warning on estrogen products covers this explicitly. The solution is equally clear: women with a uterus require a progestogen alongside estrogen. This is not optional; it is the standard of care.
Continuous combined HRT — estrogen plus progestogen taken every day — actually provides endometrial protection, with a relative risk of 0.71 (95% CI 0.56–0.90) compared to no treatment (D'Alonzo et al., 2019). The fear of endometrial cancer with HRT is largely a fear of an avoidable error in prescribing: estrogen-only HRT in a woman with a uterus. With appropriate progestogen co-administration, the endometrial cancer risk is neutralized and may even be reduced.
Women who have had a hysterectomy can safely take estrogen-only HRT, which carries a different — and generally more favorable — risk profile for both breast cancer and cardiovascular outcomes.
Who Should Not Take HRT
Eight categories of women should not take systemic HRT — these are FDA-labeled absolute contraindications, not conservative caution. Knowing them matters whether you're considering starting or already on a regimen.
The FDA's labeled contraindications for HRT include:
- Known, suspected, or personal history of breast cancer
- Known or suspected estrogen-dependent neoplasia (such as endometrial cancer)
- Active DVT, PE, or history of these conditions
- Active or recent arterial thromboembolic disease (stroke or MI within the past year)
- Undiagnosed abnormal vaginal bleeding
- Known liver impairment
- Known thrombophilic disorders (protein C, protein S, or antithrombin deficiency)
- Pregnancy
For women with a family history of breast cancer — but no personal history — the situation is not automatically a contraindication, but requires individualized risk assessment with a provider who can weigh family history, breast density, genetic risk factors, and the specific formulation and route being considered.
Women with a history of hormone-receptor-positive breast cancer should generally avoid systemic HRT. For women with other breast cancer types, the evidence is evolving and the decision requires oncology input (Deli et al., 2020).
Understanding what menopause hormone therapy can and cannot do is an important foundation before assessing your own risk picture.
FDA-labeled absolute contraindications include: personal/suspected history of breast cancer; estrogen-dependent neoplasia; active or prior DVT/PE; stroke or MI within the past year; undiagnosed vaginal bleeding; known liver impairment; thrombophilic disorders; pregnancy. Family history of breast cancer is not an automatic contraindication but requires individualized clinical assessment.
Source: FDA HRT labeling (Black Box Warnings)
Does HRT Cause Weight Gain?
HRT does not cause significant weight gain — the evidence consistently does not support this fear. What HRT does do is shift where weight sits on your body: it may reduce the central (abdominal) fat gain common during the menopausal transition and tend to preserve lean mass, so the number on the scale may stay the same while your shape changes (Arnautu et al., 2025).
The weight gain many women notice around menopause is largely driven by the hormonal transition itself — declining estrogen shifts fat distribution toward the abdomen — not by HRT. Starting HRT during perimenopause may actually attenuate this shift, though it is not a weight loss treatment. If your weight has been creeping up despite no changes in diet or exercise, the timing often correlates with the perimenopause transition rather than the HRT itself.
Progestogen Type: The Detail Your Doctor May Have Missed
The type of progestogen in your HRT matters for side effects in ways that are only recently becoming clear in clinical practice.
Synthetic progestins — like MPA (used in the original WHI formulation) and norethisterone — carry androgenic and glucocorticoid activity in addition to their progesterone action. This can contribute to mood effects, acne, and the higher breast cancer risk signals seen with testosterone-derived progestins. These are pharmacologically distinct from progesterone itself.
Oral micronized progesterone (brand names Prometrium, Utrogestan) is chemically identical to the progesterone your ovaries made. In a randomized trial of 133 women, oral micronized progesterone 300 mg nightly produced a 55% reduction in vasomotor symptoms (hot flashes) over three months. Multiple randomized trials also show it does not cause depression and improves deep sleep compared to synthetic progestins (Prior, 2018).
For women who have struggled with mood symptoms, sleep problems, or breast tenderness on synthetic progestogen-based HRT, the distinction between MPA and micronized progesterone is clinically meaningful — not just theoretical. It is worth asking your prescriber specifically which progestogen is in your regimen and why.
For more on how hormone types interact with overall hormone balance, the article on estradiol as the active form of estrogen provides useful background.
Bone Protection: A Benefit Worth Knowing
Combined HRT reduces hip fracture risk by roughly 15–29% — the most consistently proven benefit across all major HRT trials, and one that rarely gets the same attention as the cancer risk discussion.
The Cochrane review found that combined HRT reduced hip fracture risk from 111 per 1,000 women to 79–96 per 1,000 over 5.6 years — a meaningful reduction in a fracture that carries significant morbidity for postmenopausal women (Marjoribanks et al., 2017). The WHI also confirmed that both combined and estrogen-only HRT significantly reduce hip, vertebral, and total fractures (Lambrinoudaki et al., 2026).
Fracture reduction is the one HRT outcome that has consistently strong evidence across all major trials. For women at elevated fracture risk — those with low bone density, family history of osteoporosis, early menopause — this benefit may be particularly relevant to the overall risk-benefit discussion.
Frequently Asked Questions
Does HRT cause breast cancer in every woman who takes it?
No — and the absolute risk framing matters here. In the WHI, combined oral HRT (CEE+MPA) was associated with 8 additional breast cancers per 10,000 women per year compared to placebo (Rossouw et al., 2002). That is a real risk, not zero — but it is also not the same as "HRT gives you breast cancer." Estrogen-only HRT in women without a uterus showed no increase — and possibly a small reduction — in breast cancer (Lambrinoudaki et al., 2026). Progestogen type matters significantly.
Is transdermal HRT safer than pills for blood clots?
Yes, based on the best available evidence. Oral HRT carries a significantly elevated VTE risk (adjusted OR 1.58 versus no HRT), while transdermal preparations show an OR of 0.93 — essentially no increased risk (Vinogradova et al., 2019). The mechanism is first-pass liver metabolism: oral estrogen triggers clotting-factor changes that transdermal estradiol bypasses. Women with any VTE history or risk factors should discuss the transdermal route specifically.
What is the timing hypothesis for HRT safety?
The timing hypothesis holds that HRT started before age 60 or within 10 years of menopause onset carries a meaningfully different cardiovascular risk profile than HRT initiated at age 65 or later. The WHI average participant was 63 — older than the typical woman starting HRT at menopause. A 2026 reanalysis confirmed that early initiation may be cardiovascular-neutral or beneficial, while late initiation increases coronary and stroke risk (Lambrinoudaki et al., 2026). This does not mean HRT is risk-free for younger women — but the risk calculation is genuinely different.
Is micronized progesterone safer than synthetic progestins?
The breast cancer evidence favors micronized progesterone over synthetic progestins, though most supporting data comes from observational studies (particularly the large French E3N cohort) rather than head-to-head RCTs. Testosterone-derived synthetic progestins show relative risk for breast cancer of 3.35 versus estrogen alone (D'Alonzo et al., 2019), while micronized progesterone in the E3N cohort did not increase breast cancer risk (Prior, 2018). For mood, sleep, and tolerability, micronized progesterone also has a more favorable profile in randomized trials.
Can I take HRT if I have a family history of breast cancer?
A family history is not an automatic contraindication, but it does change the risk calculus and requires individualized discussion with a provider. A personal history of breast cancer is a contraindication per FDA labeling for most HRT formulations. Family history alone, without a personal diagnosis, places you in a higher-risk category that warrants detailed counseling — weighing breast density, genetic testing results (BRCA status), specific family history details, and the formulation and duration being considered. This decision cannot be made from an article alone; it needs a real clinical conversation.
Making Sense of Your Own Risk Picture
If you've read this far and feel like the picture is more complicated than you expected — that's appropriate. HRT side effects in women are real but modifiable, formulation-dependent, and highly individual.
Common early side effects — breast tenderness, bleeding irregularity, bloating — are self-limiting. Serious risks like breast cancer, VTE, and stroke are real but small in absolute terms for most women, and the route of administration and type of progestogen make a meaningful difference. When you start HRT relative to menopause changes the cardiovascular picture substantially.
The women who tend to make the best-informed decisions are those who understand both the relative and absolute risk numbers, know the difference between oral and transdermal routes, understand what their progestogen actually is, and have discussed their personal risk factors with a provider who has time to do that analysis properly.
If you're looking for that kind of conversation — one that starts with your actual labs and personal history, not a one-size-fits-all recommendation — Schedule a consultation with the HEXIS team to explore whether HRT is appropriate for your situation, which formulation makes sense, and what monitoring would look like.
For more background on how perimenopause affects hormone levels and what evidence-based treatment looks like, that article covers the transition in more depth.
The Bottom Line on HRT Side Effects
- 1
Common early symptoms (breast tenderness, spotting, bloating) are self-limiting — most resolve within 2–3 months.
- 2
The WHI's breast cancer signal was 8 extra cases per 10,000 women per year — real, but not the same as 'HRT causes breast cancer.'
- 3
Transdermal estradiol carries no significant VTE increase (OR 0.93 vs 1.58 for oral). Route matters.
- 4
The progestogen in your regimen matters: testosterone-derived progestins carry breast RR 3.35; micronized progesterone does not raise risk in the E3N cohort.
- 5
Timing matters: starting HRT before age 60 or within 10 years of menopause carries a different cardiovascular profile than late initiation.
- 6
Women with a uterus need progestogen — continuous combined HRT actually reduces endometrial cancer risk (RR 0.71).