Natural Hormone Replacement Therapy for Women: What the Evidence Actually Says
Natural Hormone Replacement Therapy for Women: What the Evidence Actually Says
The term "natural HRT" means three completely different things depending on who's selling it — and only one of them has solid clinical evidence behind it. If you've been told that compounded bioidentical hormones are safer than FDA-approved estrogen, or that black cohosh will quiet your hot flashes, you deserve a straight answer about what the research actually found.
Natural hormone replacement therapy for women covers three categories: FDA-approved body-identical estradiol and micronized progesterone, compounded bioidentical formulations (cBHRT), and plant-based options like soy isoflavones. The first category is the evidence-based starting point — supported by over 47 RCTs in 8,326 women. Compounded BHRT lacks FDA testing for safety and potency; the NASEM 2020 report found insufficient evidence to recommend it over FDA-approved alternatives. Plant-based options show modest, variable benefit that depends heavily on individual biology.
What Natural HRT Actually Means
Three categories marketed as natural — only one has FDA oversight
| Category | Example Products | FDA Status | Evidence Level |
|---|---|---|---|
Source: Sarri et al., 2017; Stuenkel et al., 2021; Pinkerton & Pickar, 2016
What "Natural" Actually Means in Hormone Therapy
"Natural" in hormone therapy means three distinct things — and only one of them, FDA-approved body-identical estradiol and micronized progesterone, has the clinical evidence and regulatory oversight to back it up.
Body-identical means the molecular structure of the hormone is identical to what your ovaries produced. Estradiol — the dominant estrogen made by human ovaries — is available as FDA-approved patches, gels, and sprays (brand names include Climara, Vivelle-Dot, and Alora). Micronized progesterone (Prometrium) is FDA-approved and chemically identical to the progesterone your body makes. These ARE the evidence-based natural options.
What they're not: conjugated equine estrogens (Premarin), which are derived from pregnant mare urine and contain estrogen compounds your body does not naturally produce. Premarin is not bioidentical — it's effective and FDA-approved, but it's a different molecule from estradiol.
Plant-derived does not mean bioequivalent. Wild yam cream, red clover extracts, and progesterone creams sold at health food stores are marketed as natural progesterone, but the human body cannot convert plant diosgenin into usable progesterone. These creams do not raise blood progesterone levels in a clinically meaningful way — a regulatory distinction confirmed by the updated medical and regulatory review of compounded hormone products (Pinkerton & Pickar, 2016). They feel natural. They do not act natural.
For a deeper look at the clinical evidence comparing different estrogen formulations, see our article on bioidentical hormone replacement therapy.
FDA-Approved Body-Identical Hormones: The Evidence-Based Starting Point
Transdermal estradiol plus micronized progesterone is the most effective treatment for vasomotor symptoms — reducing hot flash frequency to less than one-quarter of placebo rates across 47 RCTs and 8,326 women (Sarri et al., 2017). VMS affect roughly 75% of postmenopausal women, with severe symptoms in about 25% (Sarri et al., 2017).
The NICE network meta-analysis quantified that advantage precisely: a mean ratio of 0.23 (95% CrI 0.09–0.57) compared to placebo — making transdermal E+P the single most effective option across all interventions studied (Sarri et al., 2017).
Why transdermal over oral? Route matters. Oral estrogen goes through first-pass liver metabolism, which raises clotting factor levels and VTE (blood clot) risk. Transdermal estradiol bypasses the liver — it goes directly into circulation — which is why it carries a lower VTE and stroke risk profile (Files & Kling, 2020). This is one area where the "safer delivery" framing is actually supported by pharmacology.
Micronized progesterone (Prometrium) provides a cleaner profile than older synthetic progestins for most women. The KEEPS trial (Gleason et al., 2024) compared oral CEE 0.45 mg/day against transdermal estradiol 50 µg/day, with both groups using micronized progesterone 200 mg/day for 12 days per month — neither arm showed long-term cognitive harm in that randomized sample.
NASEM 2020: Compounded hormones not recommended over FDA-approved alternatives
The 2020 National Academies of Sciences, Engineering, and Medicine found insufficient evidence that compounded bioidentical hormones are safe or effective. Compounded preparations are not FDA-tested for potency, purity, or consistency — yet account for approximately one-third of all menopausal hormone prescriptions in the US.
Source: Stuenkel et al., 2021 (PMID 33739316); Santoro et al., 2021 (PMID 34482337)
Compounded Bioidentical Hormones: What the NASEM Report Found
Compounded bioidentical hormone therapy (cBHRT) is not FDA-approved, not tested for potency or purity, and is not recommended over FDA-approved alternatives — that is the conclusion of the 2020 National Academies of Sciences, Engineering, and Medicine. Despite this, cBHRT accounts for approximately one-third of all menopausal hormone prescriptions in the United States (Santoro et al., 2021). The surge followed the 2002 Women's Health Initiative results, when compounding pharmacies stepped into the gap marketing their preparations as safer and more natural — without the clinical evidence to support that claim.
What the NASEM report specifically concluded: insufficient evidence that compounded bioidentical hormones are safe or effective, and routine clinical use is not recommended over FDA-approved alternatives (Stuenkel et al., 2021). This isn't a pharmaceutical industry position — it's an independent scientific body with no financial interest in the outcome.
What specifically concerns clinicians about compounded products:
- Potency is not guaranteed. FDA-approved medications undergo rigorous manufacturing controls. Compounded preparations are not FDA-tested for content, potency, or purity. Independent testing has found real variability (Pinkerton & Pickar, 2016).
- The regulatory gap is real. Under 503A, a licensed pharmacy can legally compound patient-specific hormone preparations, but this does not mean FDA has reviewed or approved those preparations. Legal is not the same as tested.
- "Custom formulated" is not a medical advantage for most women. Marketed as precisely tailored, cBHRT formulations — especially pellets with fixed doses — often cannot be adjusted after insertion. That's less flexibility, not more.
If you're seeking body-identical estradiol and micronized progesterone, FDA-approved versions (Climara patch, Prometrium capsules) give you those exact molecules with the same testing, manufacturing controls, and pharmacovigilance data that all approved drugs carry.
Phytoestrogens: Soy Isoflavones and What the Research Actually Shows
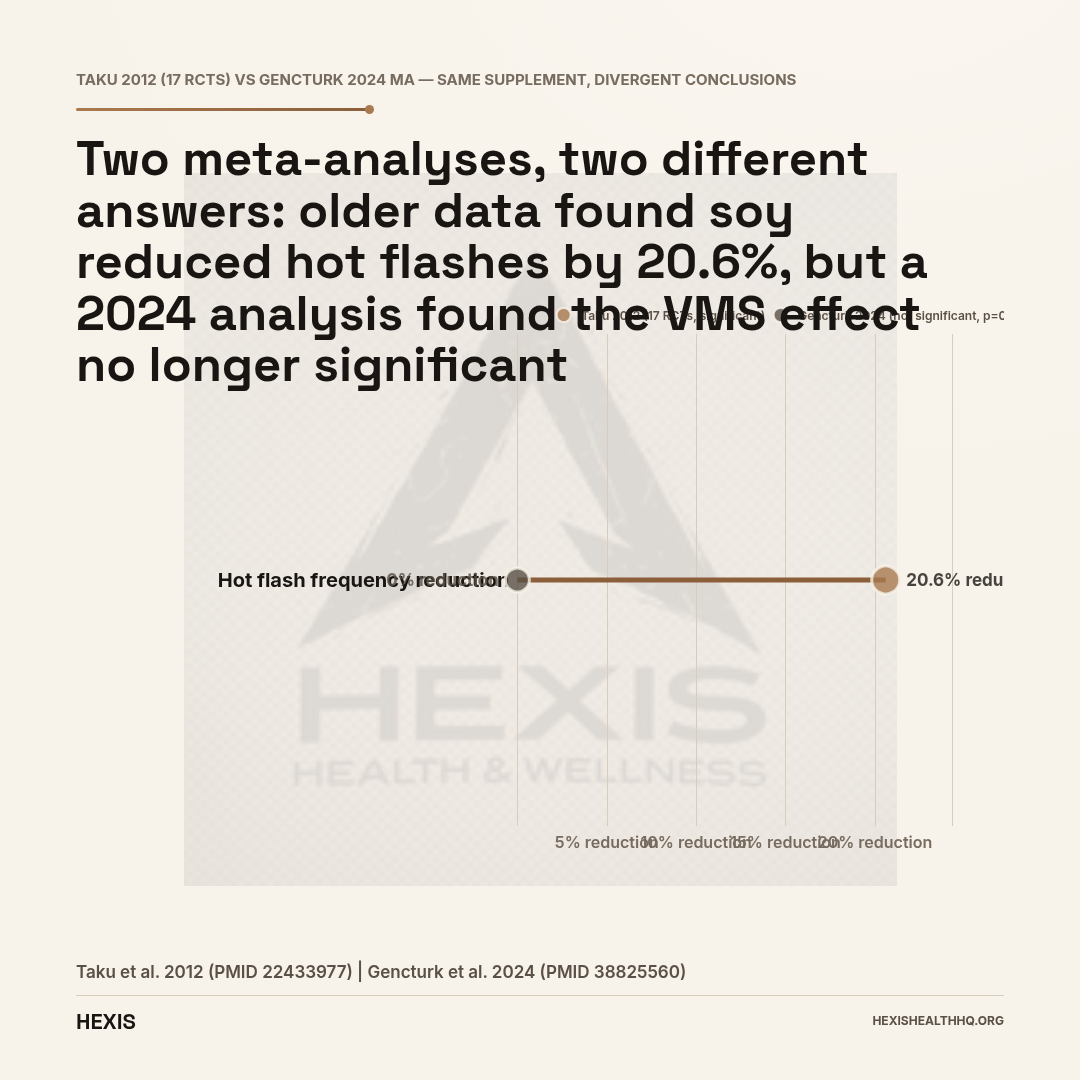
Soy isoflavones show modest, mixed results for menopausal symptoms — older meta-analyses found about a 20% reduction in hot flash frequency, while a 2024 meta-analysis found the VMS effect no longer statistically significant. They are the most studied plant-based option, and whether you benefit depends heavily on your individual biology, specifically whether you produce the metabolite equol.
The older data looked promising. A systematic review and meta-analysis of 17 RCTs (Taku et al., 2012) found that soy isoflavones reduced hot flash frequency by 20.6% and hot flash severity by 26.2% compared to placebo. Statistically significant. Clinically modest.
The 2024 data is more cautious. A more recent meta-analysis (Gençtürk et al., 2024) that analyzed VMS outcomes found that the effect of soy isoflavones was NOT statistically significant — SMD of -0.49 (p=0.14). The same analysis did find a significant effect on depressive symptoms (SMD -0.41, p=0.01) — relevant for women whose primary concern is mood during menopause.
Equol-producer status changes the picture. About 30–50% of Western women produce equol, a metabolite of daidzein that has stronger estrogenic activity than the parent compound. A meta-analysis of six RCTs (Daily et al., 2019) found that equol-producer status significantly predicted whether soy isoflavones would help. If you're not an equol producer, the benefit is likely minimal.
On safety: soy isoflavones do not significantly thicken the endometrium in postmenopausal women — that concern was examined in a systematic review (Teixeira et al., 2022) and the evidence does not support clinically meaningful estrogenic endometrial effects at typical supplement doses. However, the picture for women with a history of breast cancer is more complex and unsettled; that population should discuss soy supplementation directly with their oncologist.
The practical takeaway: soy isoflavones at around 54 mg/day aglycone equivalent (the median effective dose from Taku et al., 2012) may offer modest benefit if you're in the equol-producing subgroup. It's a reasonable low-risk option to try if you can't or won't use hormone therapy. It is not a replacement for estradiol in women with significant VMS.
Does Black Cohosh Work for Hot Flashes?
Black cohosh (Cimicifuga racemosa) does not outperform placebo in the best-controlled clinical evidence — despite being one of the most purchased herbal supplements for menopause.
A well-designed RCT (Tanmahasamut et al., 2015) compared black cohosh extract at 40 mg/day against placebo in 54 women over 8 weeks. The result: no significant difference in menopausal symptom scores (p=0.174). Not a small trial done badly — a controlled, randomized study using the standardized dose most often recommended.
An overview of systematic reviews on complementary approaches to VMS (Guo et al., 2019) found mixed and largely low-quality evidence for black cohosh, consistent with the RCT picture.
The safety profile of black cohosh at 40 mg is generally acceptable — the Tanmahasamut study saw no serious adverse events or liver function changes. But acceptable safety combined with no demonstrated efficacy doesn't add up to a treatment recommendation.
If you're using black cohosh because you've heard it works: the data says it probably doesn't, at least not meaningfully more than placebo.
Cardiovascular Considerations and Route of Administration
Transdermal estrogen carries a lower VTE and stroke risk than oral estrogen because it bypasses first-pass liver metabolism — oral estrogen raises clotting factor and triglyceride levels; transdermal does not (Files & Kling, 2020). This is why transdermal delivery is preferred for women with cardiovascular risk factors, a history of migraines with aura, or older age at initiation.
Cardiovascular risk from MHT is also heavily influenced by timing — the "timing hypothesis" suggests that benefits are greater and risks lower when therapy is started within 10 years of menopause or before age 60. This comes up in every major guideline update, and it's why blanket statements about HRT being dangerous tend to mislead: the risk-benefit calculation is highly individual and depends substantially on age, timing, and formulation choice.
For the broader picture of HRT risk-benefit in menopause, our article on HRT for menopause covers the evidence in more depth. Women navigating perimenopause specifically may also find our guide on perimenopause symptoms and treatment useful for understanding where in the hormonal transition they fall.
“Soy isoflavones at around 54 mg/day may offer modest benefit if you are in the equol-producing subgroup. It is a reasonable low-risk option to try if you cannot or will not use hormone therapy. It is not a replacement for estradiol in women with significant VMS.”
Plant-Derived Lipid Supplements and Bone/Cardiovascular Outcomes
Phytoestrogens show real, if modest, benefits on lipid profiles in postmenopausal women — a secondary effect beyond VMS that matters for women managing cardiometabolic risk alongside menopausal symptoms. A 2022 systematic review and meta-analysis (Blaszczuk et al., 2022) found that flaxseed, soy, and red clover supplementation were associated with favorable changes in lipid profiles — specifically lower LDL and total cholesterol. The cardiovascular implications are not established as equivalent to those of FDA-approved hormone therapy.
A 2025 updated meta-analysis (Park et al., 2025) of plant-derived dietary supplements in menopausal women confirmed modest lipid-lowering effects across a range of formulations. These aren't dramatic benefits, but they are consistent enough to be relevant for women who need non-hormonal options and have cardiovascular risk factors to manage.
Frequently Asked Questions
Is bioidentical HRT safer than conventional HRT?
FDA-approved bioidentical estradiol (patches, gels) and micronized progesterone (Prometrium) have a well-characterized safety profile from decades of clinical use and large trials. They are not inherently safer than all conventional options — the safety difference is primarily between oral and transdermal delivery routes, not between "bioidentical" and "conventional" as broad categories.
What is the difference between compounded and FDA-approved bioidentical hormones?
Both can contain identical hormones — estradiol and progesterone. The difference is oversight. FDA-approved versions are tested for potency, purity, and consistency. Compounded preparations are not FDA-tested. The NASEM 2020 report concluded there is insufficient evidence that compounded bioidentical hormones are safe or effective, and they are not recommended routinely over FDA-approved alternatives (Stuenkel et al., 2021).
Does black cohosh really work for hot flashes?
The best-controlled evidence says no. A randomized trial of black cohosh 40 mg/day versus placebo in 54 women found no significant difference in menopausal symptoms (p=0.174) (Tanmahasamut et al., 2015). It's generally safe at this dose, but the efficacy data does not support it as a meaningful treatment for VMS.
Are soy isoflavones effective for menopause symptoms?
Results are modest and variable. Older meta-analyses found about a 20% reduction in hot flash frequency (Taku et al., 2012), but a 2024 meta-analysis found the VMS effect was not statistically significant (SMD -0.49, p=0.14) (Gençtürk et al., 2024). Efficacy depends significantly on whether you produce equol, a soy metabolite — only about 30–50% of Western women do (Daily et al., 2019). Worth trying as a low-risk option; not a replacement for estradiol in severe cases.
Is plant-based progesterone cream the same as prescription progesterone?
No. Over-the-counter progesterone creams made from wild yam or other plant sources cannot be converted to biologically active progesterone by the human body. They will not raise serum progesterone levels in a clinically meaningful way and do not protect the uterine lining the way prescription micronized progesterone does. If you need progesterone, you need the prescription form.
What This Means for Your Next Conversation With a Provider
If you want natural hormone replacement therapy and what you actually mean is evidence-based, body-identical hormones with the lowest-risk profile, that exists — it's FDA-approved transdermal estradiol and oral micronized progesterone. Start there.
If you're drawn to compounded hormones, it's worth asking your provider specifically what those offer that FDA-approved alternatives don't. In most cases, the honest answer is: nothing testable.
If you're not ready for hormone therapy, soy isoflavones at 54 mg/day are a reasonable, safe, modest option — with realistic expectations. Black cohosh is probably not worth your money.
The conversation worth having is an individualized one: your labs, your symptoms, your health history, and your risk profile. That's where treatment decisions actually get made.
At HEXIS, every protocol starts with labs — not assumptions about what category of treatment is "more natural." If you want a physician-guided evaluation of your options, schedule a consultation.
- 1
FDA-approved body-identical estradiol (patches, gels) and micronized progesterone (Prometrium) are the evidence-based natural option — same molecules, FDA-tested for potency and purity.
- 2
Compounded BHRT uses the same hormones but lacks FDA oversight. NASEM 2020 found insufficient evidence it is safer or more effective than FDA-approved alternatives.
- 3
Soy isoflavones offer modest benefit for some women. A 2024 meta-analysis found VMS effects no longer statistically significant; equol-producer status (~30-50% of Western women) predicts who benefits.
- 4
Black cohosh did not outperform placebo in the best RCT (p=0.174, n=54). Safe — but efficacy is not demonstrated.
- 5
Wild yam cream and OTC progesterone creams do not raise serum progesterone. Not equivalent to prescription micronized progesterone.