Hormone Replacement Therapy for Menopause: What the Evidence Actually Says
Hormone Replacement Therapy for Menopause: What the Evidence Actually Says
For over two decades, millions of women avoided HRT because of a single study published in 2002. That study scared everyone — including most doctors. The problem is that the alarm was based on women who were, on average, 63 years old, more than a decade past menopause, and using a specific oral hormone combination. If you're in your late 40s or early 50s dealing with hot flashes, night sweats, brain fog, or vaginal dryness, that data does not apply to you.
Here's what the current evidence actually says about hormone replacement therapy for menopause: started at the right time, in the right form, for the right person, it is one of the most effective and well-studied treatments in medicine. At HEXIS, we work through this conversation with patients regularly — the misapplication of the 2002 WHI data remains the single most common reason women delay treatment they would benefit from.
The short answer: HRT — estrogen alone or combined with progesterone — is FDA-approved for vasomotor symptoms (hot flashes, night sweats), genitourinary syndrome of menopause (GSM), and osteoporosis prevention. For women under 60 or within 10 years of their last period with no contraindications, the benefits consistently outweigh the risks. Route of delivery matters — transdermal estradiol and micronized progesterone carry lower risks than older oral formulations (Chester et al., 2018).
What Is HRT for Menopause, and What Is It Approved For?
Hormone replacement therapy for menopause replaces the estrogen (and often progesterone) your ovaries stop producing as you enter and complete menopause. It is not a fringe treatment or a gray-area supplement. Estradiol, conjugated estrogens, and micronized progesterone are all FDA-approved medications with decades of safety and efficacy data.
The FDA has approved these therapies for three specific indications:
- Vasomotor symptoms — the hot flashes and night sweats that wake you up at 2am and soak through your clothes during meetings
- Genitourinary syndrome of menopause (GSM) — vaginal dryness, painful sex, urinary urgency, and recurrent UTIs caused by declining estrogen
- Osteoporosis prevention — estrogen plays a direct role in bone maintenance; losing it accelerates bone density loss
If you have a uterus, you need progesterone alongside estrogen to protect your endometrium. If you've had a hysterectomy, estrogen alone is the protocol. This is not optional — it's a basic structural requirement of combined HRT (Davis & Baber, 2022).
The WHI Study: What It Actually Found (and What It Didn't)
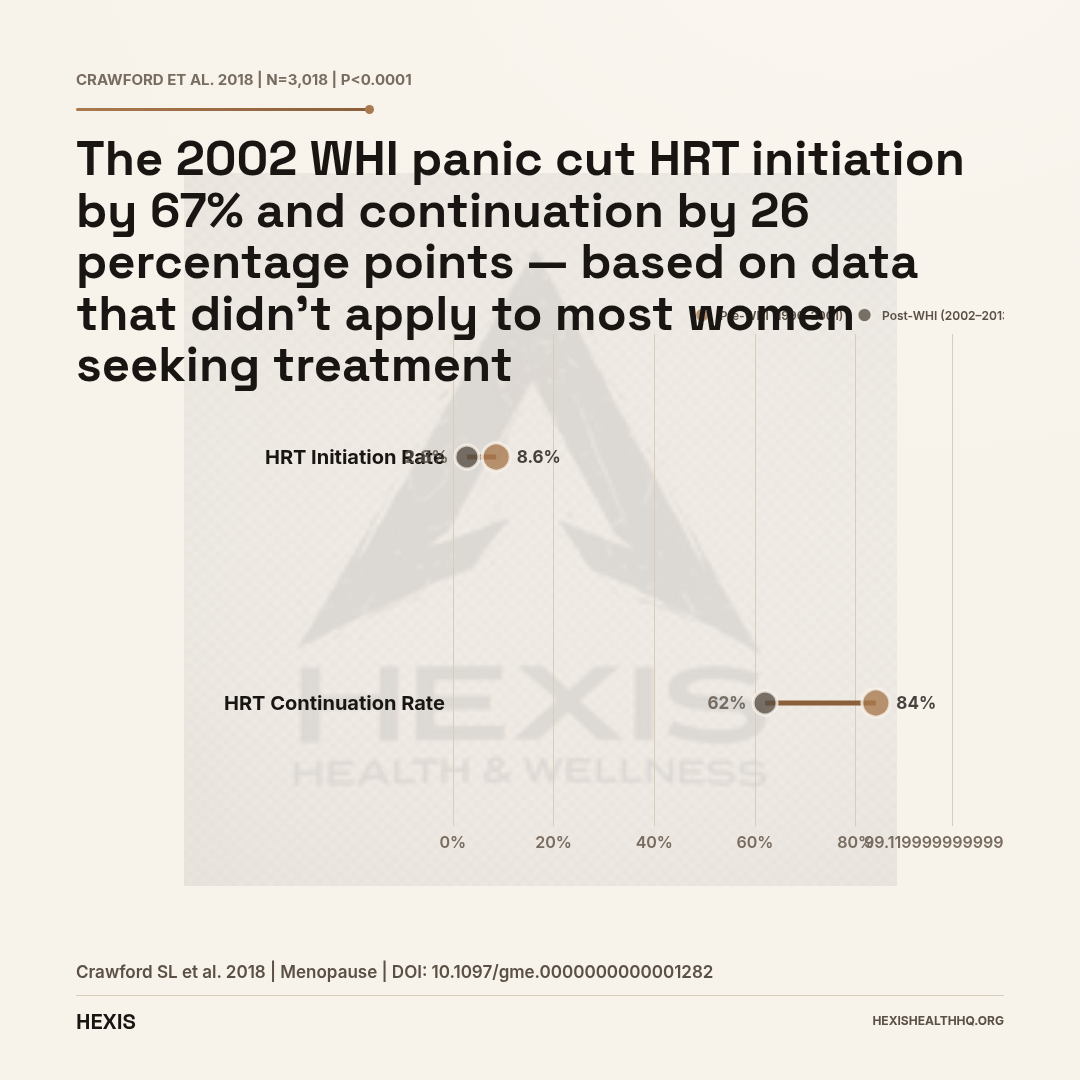
In 2002, the Women's Health Initiative (WHI) trial was stopped early and dominated every headline. HRT prescriptions collapsed. Between 1996–2001 (pre-WHI), 8.6% of women in the study cohort were initiating HRT. By 2002–2013, that dropped to 2.8% — a more than two-thirds reduction, statistically significant at p<0.0001 across 3,018 participants (Crawford et al., 2018). Continuation rates dropped from 84.0% to 62.0% over the same period (Crawford et al., 2018).
The panic made sense given the headlines. The research, looked at more carefully, tells a more complicated story.
The WHI enrolled women with an average age of 63 — many of them more than a decade past menopause. The formulation studied was oral conjugated equine estrogens plus medroxyprogesterone acetate (Provera), a synthetic progestin. When the data was re-analyzed stratified by age and time since menopause, a very different picture emerged: women who started HRT under age 60 or within 10 years of menopause showed reduced cardiovascular mortality and all-cause mortality, not increased risk (Chester et al., 2018).
This reanalysis is now called the timing hypothesis or the window of opportunity.
The Timing Hypothesis: Starting Early Changes Everything
Estrogen appears to protect the cardiovascular system when blood vessels are healthy, but can cause problems when atherosclerosis is already established. Starting HRT in the years just after menopause — when arteries are still responsive — is a fundamentally different situation from starting it a decade later.
Women who initiated HRT after age 60 or more than 10 years post-menopause showed a different risk profile than early starters. This is why current NAMS (North American Menopause Society) guidance, endorsed by the American College of Obstetricians and Gynecologists, recommends initiating therapy before age 60 or within 10 years of menopause for women with bothersome symptoms and no contraindications (Davis & Baber, 2022).
“Women who started HRT under age 60 or within 10 years of menopause showed reduced cardiovascular mortality and all-cause mortality, not increased risk.”
What Are the Real Benefits of HRT?
Vasomotor Symptoms (Hot Flashes and Night Sweats)
Estrogen therapy is the most effective treatment available for vasomotor symptoms — full stop. Nothing else tested comes close to its efficacy. We're talking about the symptom that disrupts sleep, impairs concentration, affects mood, and drives more menopause-related healthcare visits than anything else.
If you're waking up multiple times a night drenched in sweat, or if you're having 8-10 hot flashes per day, non-hormonal options (SSRIs, gabapentin, fezolinetant) can help — but they work less well and carry their own side effect profiles. HRT is the first-line option when there are no contraindications (Niskanen et al., 2025).
Bone Protection
Estrogen keeps bone-resorbing cells (osteoclasts) in check. When estrogen falls at menopause, bone loss accelerates — rapidly at first, then more slowly. HRT directly slows this process.
A 2021 review in Best Practice & Research: Clinical Endocrinology & Metabolism confirmed that MHT preserves bone mineral density and reduces fracture risk at the hip, spine, and wrist (Gosset et al., 2021). The protection lasts only as long as treatment continues — bone loss resumes after stopping, which is a key reason individual duration decisions matter.
HRT is most appropriate for bone protection in women who also have symptomatic menopause and are already taking it — not as a standalone osteoporosis drug when asymptomatic, where bisphosphonates are typically preferred (Rozenberg et al., 2020).
Genitourinary Syndrome of Menopause (GSM)
GSM — vaginal dryness, atrophy, painful intercourse, urinary urgency — affects the majority of postmenopausal women and, unlike hot flashes, does not improve with time. It gets worse.
A 2026 randomized controlled trial published in Maturitas specifically examined the effect of hormone therapy on vaginal microbiota in women with GSM (Panyakhamlerd et al., 2026). The results showed that systemic HRT altered the vaginal microbiome toward a healthier lactobacillus-dominant profile — a direct mechanism by which estrogen restores vaginal tissue health.
Local vaginal estrogen (low-dose cream, ring, or tablet) can treat GSM with minimal systemic absorption and is often appropriate even for women who can't use systemic HRT.
Musculoskeletal Benefits: Discs, Tendons, and Joints
One underappreciated area is HRT's effect on the musculoskeletal system beyond bone density.
In a 2023 RCT published in Climacteric, Stevenson et al. measured intervertebral disc height in 355 postmenopausal women randomized to oral estradiol or placebo. Women taking 1 mg estradiol daily showed a +0.16 cm increase in disc height over 2 years (p=0.015), while women on 2 mg showed a +0.21 cm increase (p=0.006) (Stevenson et al., 2023). Small numbers, real signal — the discs that compress as estrogen declines appear to partially recover.
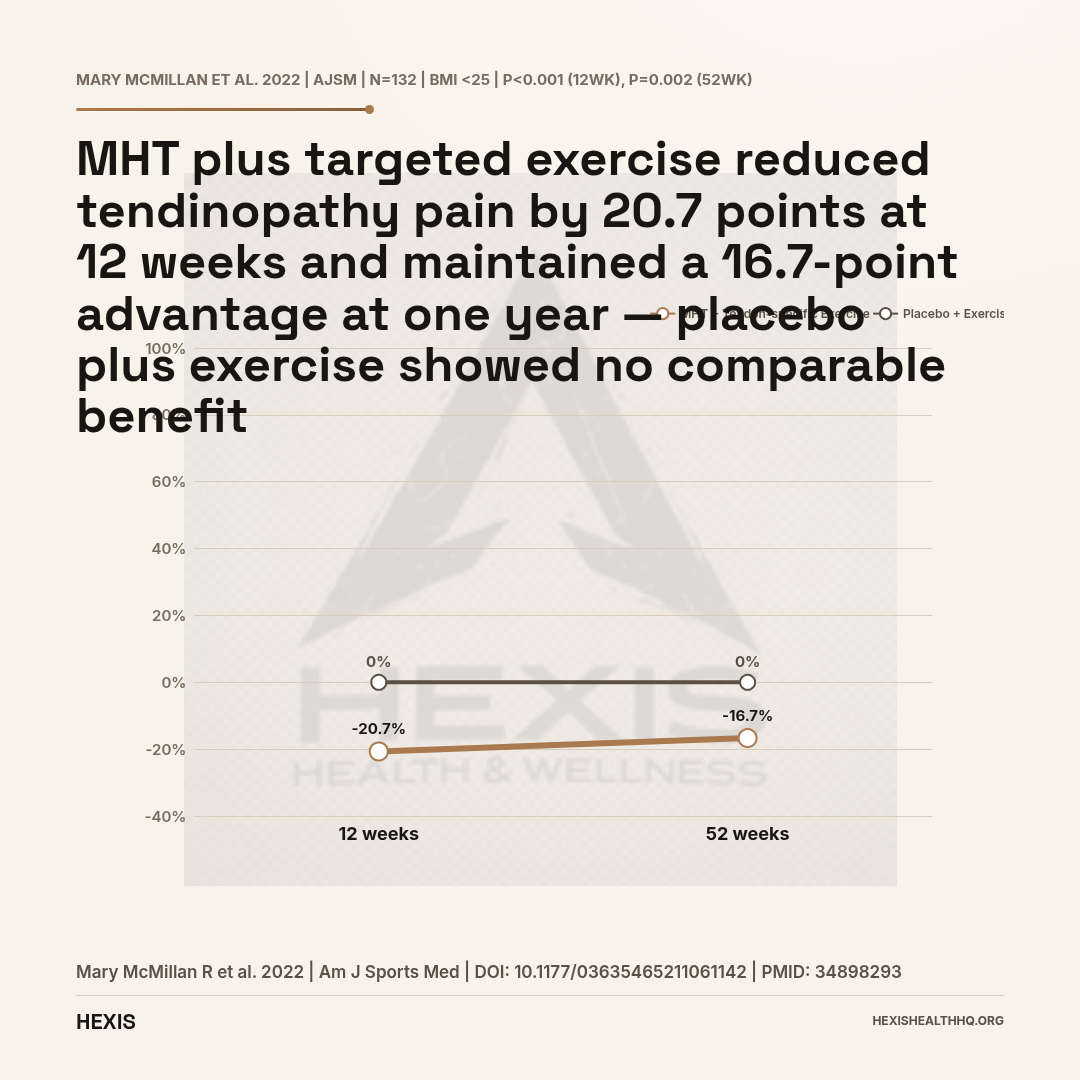
On the tendon side, a 2022 RCT in The American Journal of Sports Medicine by Mary McMillan et al. enrolled 132 postmenopausal women with greater trochanteric pain syndrome. Women with BMI under 25 who received MHT combined with tendon-specific exercise showed a VISA-G score improvement of −20.72 points at 12 weeks (95% CI −31.22 to −10.22; p<0.001) and −16.71 points at 52 weeks (95% CI −27.21 to −6.22; p=0.002) compared to exercise plus placebo (Mary McMillan et al., 2022). That's a clinically meaningful reduction in tendinopathy pain sustained at one year.
And in a 2025 study in Women's Health, Sasaki et al. found MHT outperformed complementary and alternative medicine for hand osteoarthritis symptoms in perimenopausal women (Sasaki et al., 2025).
Brain and Cognition
This is where the science is actively evolving — and where the timing hypothesis applies again.
The KEEPS Continuation Study (a long-term follow-up of the Kronos Early Estrogen Prevention Study) published in 2024 in PLoS Medicine found no significant difference in cognitive outcomes between women who took MHT early in menopause versus those who took placebo — but also found no harm (Gleason et al., 2024). The finding is reassuring for early starters.
A 2026 study in Alzheimer's & Dementia from the same KEEPS cohort went further, examining amyloid PET and MRI outcomes. Kantarci et al. found that women who started oral CEE (conjugated equine estrogen) early in menopause had lower white matter hyperintensity volumes years later, suggesting a possible protective effect on brain aging (Kantarci et al., 2026). This is preliminary but important data.
A separate 2025 review in The Journal of Clinical Endocrinology and Metabolism by Mosconi et al. examined the mechanistic links between menopause, MHT, and Alzheimer's disease risk — noting that the timing of initiation and the type of estrogen used may matter significantly (Mosconi et al., 2025).
Starting HRT early in menopause looks neurologically safe and possibly protective. Starting it decades later in women with established dementia pathology is a different question — and the current data doesn't give optimistic answers there.
What Are the Real Risks of HRT?
Breast Cancer
This is the number that scares most people, and it deserves a straight answer.
Combined estrogen-progestogen therapy (EPT) is associated with a small increased risk of breast cancer — roughly 1 additional case per 1,000 women per year of use. That number is real and statistically significant, and you should weigh it when making this decision (Rozenberg et al., 2021).
Estrogen-only therapy (ET), used in women who've had a hysterectomy, does not show the same increased risk. In the WHI estrogen-only arm, breast cancer rates were actually slightly lower in the HRT group than in the placebo group, though that finding didn't reach significance.
The type of progestogen matters. Micronized progesterone (Prometrium, identical in structure to your body's own progesterone) appears to carry a lower breast cancer risk than synthetic progestins like medroxyprogesterone acetate — the compound used in the original WHI (Davis & Baber, 2022). This is a clinically important distinction that most people don't hear.
Blood Clots (VTE) and Stroke
Oral estrogen increases VTE (venous thromboembolism) risk by roughly 2-fold over baseline — but baseline risk in healthy menopausal women is already low, so the absolute numbers are small.
Transdermal estradiol (patch, gel, spray) bypasses first-pass liver metabolism and does not appear to increase VTE or stroke risk at standard doses. This is a consistent finding across multiple observational studies and meta-analyses (Anagnostis et al., 2019). It's one of the strongest arguments for choosing transdermal over oral for most women, especially those with any personal or family history of clotting.
The same route-of-delivery principle applies to progestogens: micronized progesterone has a more favorable clot and stroke profile than synthetic progestins (Davis & Baber, 2022).
Cardiovascular Risk: The Full Picture
In healthy women under 60 who start HRT early, cardiovascular outcomes are generally neutral to favorable. The timing hypothesis holds: cardioprotection when started in the window, potential harm when started late in women with already-established disease (Anagnostis et al., 2019).
The 2022 review in Nature Reviews Endocrinology (Davis & Baber, 2022) summarizes the current consensus: MHT initiated in younger, healthy postmenopausal women does not increase CHD risk and may reduce it. The excess risk seen in older WHI participants should not be extrapolated to women starting HRT at 48.
- ER-positive (hormone receptor-positive) breast cancer history — systemic estrogen is contraindicated
- Active or recent venous thromboembolism (VTE) or stroke
- Unexplained vaginal bleeding
- Active liver disease
Source: Armeni et al., Best Practice & Research, 2021
Who Is a Candidate for HRT?
You're likely a good candidate if:
- You have bothersome vasomotor symptoms (hot flashes, night sweats) disrupting sleep or daily function
- You have GSM symptoms (vaginal dryness, painful sex, urinary urgency)
- You're under age 60 or within 10 years of your last period
- You have no contraindications (see below)
- You want osteoporosis prevention alongside symptom relief
The 2025 IMS World Congress guidance confirms this candidacy framework, emphasizing that HRT initiation within the window of opportunity offers the best risk-benefit balance (Simon et al., 2025).
Who Should Not Take HRT
Hard contraindications include:
- ER-positive (hormone receptor-positive) breast cancer history — systemic estrogen is contraindicated. Local vaginal estrogen may still be an option in select cases; discuss with your oncologist.
- Active or recent VTE or stroke
- Unexplained vaginal bleeding
- Active liver disease
Women with a history of blood clots may still be candidates for transdermal estradiol with close monitoring — the route distinction matters here too (Armeni et al., 2021).
HRT for Women With POI
Women with primary ovarian insufficiency (POI) — natural or surgical — who reach menopause before 40 face decades without estrogen protection for their hearts, bones, and brains. For these women, HRT is strongly recommended until at least the average age of natural menopause (Sullivan et al., 2016). The risk-benefit calculation is fundamentally different when you're 32 and losing estrogen than when you're 55.
HRT Route and Type: How They Compare
Source: Davis & Baber, Nature Reviews Endocrinology, 2022; Anagnostis et al., 2019
What Form of HRT Is Safest?
Route and type both matter. Here's what the evidence shows:
Transdermal estradiol (patch, gel, spray) is generally preferred over oral estrogen for most women because it avoids the liver's first-pass processing and does not increase clot risk the way oral estrogen does. The dose is 0.025–0.1 mg/day via patch, adjusted based on symptom control.
Oral estradiol (0.5–2 mg/day) or conjugated equine estrogens are effective but carry a modestly higher VTE and stroke risk than transdermal — particularly relevant for women with risk factors.
Micronized progesterone (Prometrium, 100–200 mg/day for women with a uterus) is the preferred progestogen. It's bioidentical in structure to the body's own progesterone and has a more favorable safety profile for both breast cancer and cardiovascular risk compared to synthetic progestins. This is an FDA-approved medication — not a compounded product.
Local vaginal estrogen (low-dose cream, ring, or suppository) is appropriate for isolated GSM with minimal systemic absorption. It can often be used even when systemic HRT is not appropriate.
Compounded "Bioidentical" HRT
There's a lot of confusion here. The term "bioidentical" is a marketing term, not a regulatory category. FDA-approved estradiol (transdermal patch, gel) and micronized progesterone are bioidentical in the true sense — their molecular structure is identical to what your body makes. They're also standardized, tested for potency and sterility, and covered by insurance.
Compounded BHRT (from 503A pharmacies) is not FDA-approved for safety or efficacy. Potency and sterility can vary between batches. In some cases, compounded formulations may be useful when a specific dose or delivery form isn't commercially available — but this should be a targeted decision, not a default (Arnautu et al., 2025).
How Long Can You Stay on HRT?
The old "5-year rule" is not evidence-based. It came from early, overcautious guidelines shaped by the 2002 WHI panic — the same panic that drove HRT continuation rates from 84.0% down to 62.0% in the decade after 2002 (Crawford et al., 2018).
NAMS 2022 states clearly: there is no evidence-based reason to impose an arbitrary stopping age or duration limit on HRT. Duration should be individualized based on symptom burden, risk factors, and patient preference — with regular reassessment (Lundberg et al., 2020).
Some women need HRT for a few years to get through the acute symptomatic phase. Others have ongoing symptoms into their 60s and 70s and benefit from continued therapy. For women with GSM, symptoms don't resolve spontaneously and local or systemic therapy may be appropriate indefinitely.
If you do decide to stop, gradual tapering is generally preferred over abrupt discontinuation to reduce symptom rebound — though the evidence on optimal tapering protocols is limited.
FAQ
Is HRT safe after everything the WHI study found?
For most women under 60 who start within 10 years of menopause, yes — the benefits outweigh the risks. The WHI alarm applied to older women using an older oral formulation. Current guidance from NAMS, ACOG, and the IMS supports HRT for eligible women with bothersome symptoms, using transdermal estradiol and micronized progesterone when possible to minimize risks.
Does HRT cause blood clots?
Oral estrogen does modestly increase clot risk. Transdermal estradiol does not appear to at standard doses — a consistent finding across multiple studies. Women with personal or family history of VTE should discuss transdermal routes specifically (Anagnostis et al., 2019).
How do I know if I need progesterone with my estrogen?
If you have a uterus, you need progestogen to protect your endometrium from estrogen-driven overgrowth. Estrogen-only therapy is reserved for women who've had a hysterectomy. Micronized progesterone is the preferred option when a progestogen is needed.
Can HRT help with brain fog and mood?
It can, particularly for brain fog and mood disruption that's tied to sleep disruption from hot flashes and night sweats. Direct cognitive effects are still being studied. The KEEPS Continuation Study found no significant cognitive harm from early MHT use — and some imaging data from Kantarci et al. (2026) suggests possible brain-protective effects of early estrogen exposure. Starting HRT in the menopausal window appears to be safe for the brain.
When should I start — and when should I stop?
Start when you have bothersome symptoms and you're within the window: under 60 or within 10 years of your last period. Stop when you and your provider decide the risk-benefit balance has shifted — not based on an arbitrary time limit. Reassess annually. NAMS explicitly states there is no evidence-based cutoff at age 65.
What HEXIS Does Differently
HRT decisions aren't one-size-fits-all, and they shouldn't be rushed. At HEXIS, every protocol starts with a complete hormone panel — not a symptom checklist. Your provider will review your estradiol, FSH, LH, progesterone, testosterone, thyroid, and metabolic markers before recommending anything.
If you're a candidate, we'll talk through the options: transdermal versus oral, bioidentical versus synthetic progestogens, systemic versus local. Your estradiol level, FSH, lipid panel, and clotting history all shape which route makes sense — a woman with a personal history of DVT gets a very different conversation than one without. We explain the real risk numbers — not a panic from 2002, and not a sales pitch either.
If you're in Great Falls or anywhere in Montana, Idaho, Washington, or Oregon, you can see a HEXIS provider via telehealth. Schedule a consultation to start with your labs.
You may also find these related articles useful: perimenopause symptoms and treatment, testosterone for women, and low testosterone symptoms in men.
- 1
The 5-year rule came from overcautious guidelines after the 2002 WHI panic — not from evidence
- 2
NAMS 2022: no arbitrary stopping age or duration limit. Reassess annually based on your symptoms and risk profile
- 3
Women with ongoing vasomotor symptoms or GSM may benefit from continued therapy into their 60s and 70s
- 4
If you stop, gradual tapering reduces symptom rebound — though optimal taper protocols aren't yet well-defined
- 5
Start a conversation with your provider: the right duration is individual, not a calendar event