Estradiol Patch: Dosing, Placement & Side Effects
Estradiol Patch: Dosing, Placement & Side Effects
Your doctor hands you a prescription for an estradiol patch and sends you on your way. Maybe they mentioned hot flashes. Maybe they said something about hormones. What they probably did not explain: how much estradiol you're actually getting, where the patch should go, why location changes how much you absorb, or what separates this form of HRT from the oral pill sitting in most pharmacies. That gap is what this article fills.
The estradiol patch delivers 17-beta estradiol through your skin at 0.014–0.1 mg/day. Because it bypasses the liver, it does not raise clotting factors the way oral estrogen does — a key VTE advantage. FDA-approved for vasomotor symptoms and osteoporosis prevention. Most women start at 0.025–0.05 mg/day and titrate from there.
Reviewed by the HEXIS Medical Team — physicians board-certified in internal medicine and hormone optimization. All clinical data cited from peer-reviewed journals; see Sources.
What Estradiol Patch Brands Are FDA-Approved?
Several estradiol patch formulations are FDA-approved for menopausal hormone therapy in the United States. You'll most commonly encounter:
- Climara — once-weekly patch, available from 0.025 to 0.1 mg/day
- Vivelle-Dot — twice-weekly, available from 0.025 to 0.1 mg/day
- Minivelle — twice-weekly, small-format patch, 0.025 to 0.1 mg/day
- Alora — twice-weekly, 0.025 to 0.1 mg/day
- Menostar — once-weekly, ultra-low dose at 0.014 mg/day (osteoporosis prevention only, not approved for hot flash treatment)
All deliver 17-beta estradiol — the same estrogen your ovaries made before menopause. Generic transdermal estradiol systems are also available. The choice between brands often comes down to patch size preference, change schedule, and how your skin reacts (Ibarra de Palacios et al., 2002). For a broader look at how all these HRT options compare, see our guide to hormone replacement therapy for women.
What Dosing Strengths Are Available?
The available patch strengths, from lowest to highest delivery rate, are:
| Dose (mg/day) | Common Brand | Indication |
|---|---|---|
| 0.014 | Menostar | Osteoporosis prevention only |
| 0.025 | Climara, Vivelle-Dot, Minivelle, Alora | Vasomotor symptoms, osteoporosis |
| 0.0375 | Climara, Vivelle-Dot | Vasomotor symptoms, osteoporosis |
| 0.05 | Climara, Vivelle-Dot, Minivelle, Alora | Vasomotor symptoms, osteoporosis |
| 0.075 | Climara, Vivelle-Dot | Vasomotor symptoms, osteoporosis |
| 0.1 | Climara, Vivelle-Dot | Vasomotor symptoms, osteoporosis |
Most prescribers start at 0.025–0.05 mg/day and titrate based on symptom response and serum estradiol levels (Sriprasert et al., 2020). The goal is the lowest dose that controls your symptoms effectively.
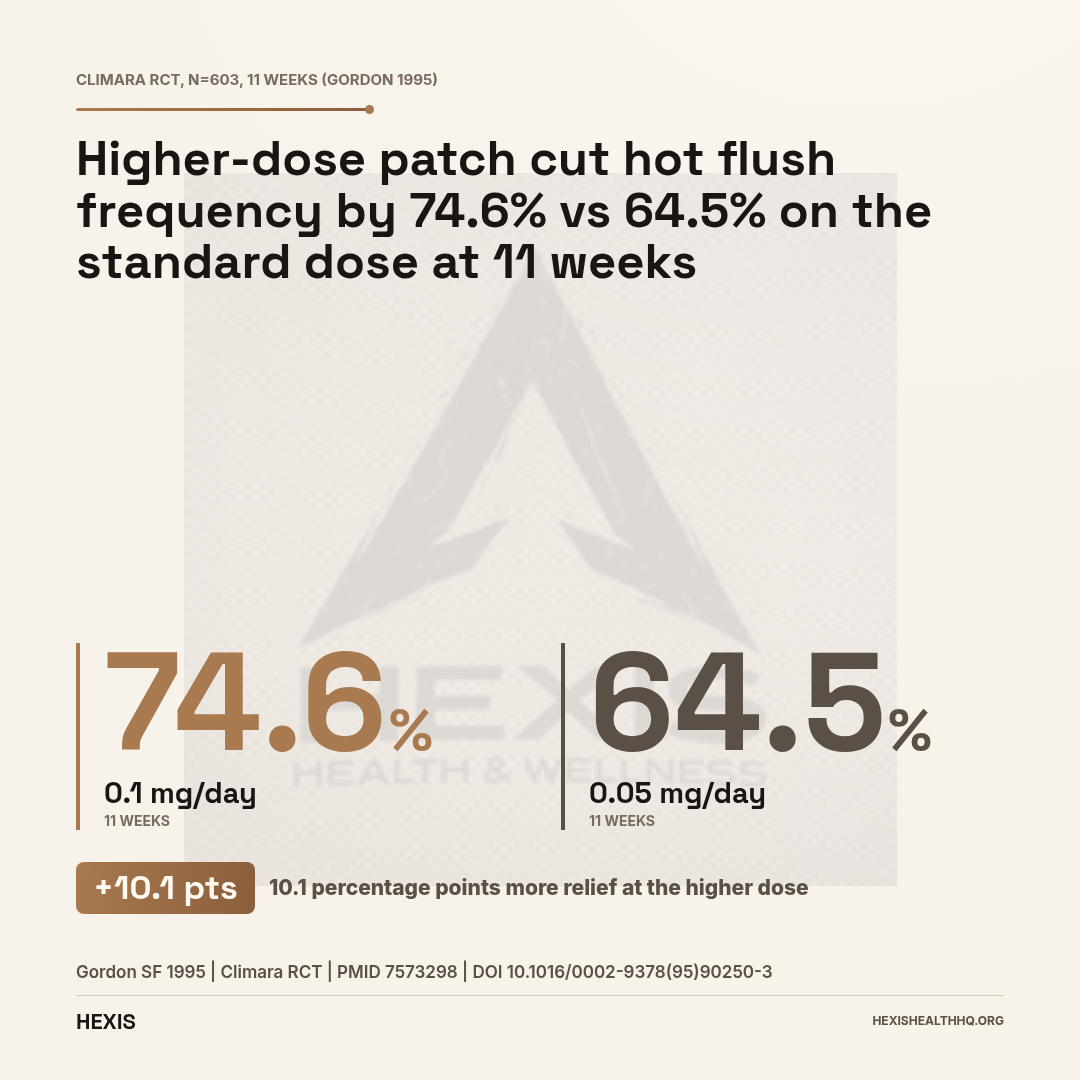
In the pivotal Climara RCT (n=603), women on the 0.1 mg/day patch achieved a 74.6% reduction in hot flush frequency at 11 weeks, compared to 64.5% on the 0.05 mg/day patch (Gordon, 1995). That dose-response relationship is real — higher doses tend to work better for vasomotor symptoms, but they also carry a modestly higher side effect burden, particularly around breast tenderness. Starting lower and moving up gives your body time to adjust.
Absorption by Application Site (Climara Patch)
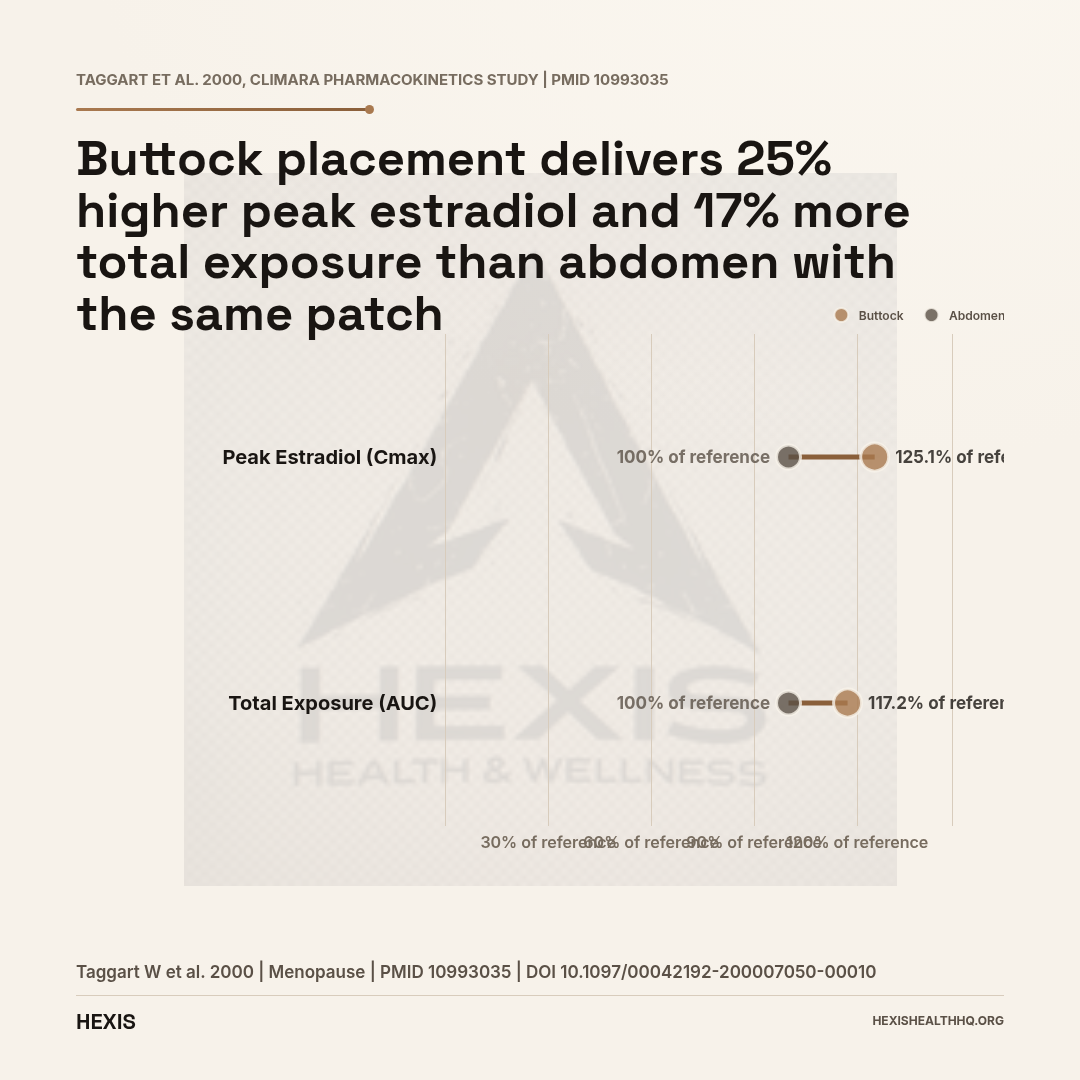
Same patch, same dose — location changes how much estradiol enters circulation (Taggart et al., 2000)
| Site | Cmax (vs. abdomen) | AUC (vs. abdomen) |
|---|---|---|
Does Patch Placement Actually Matter?
Yes — and this is one of the most underappreciated facts about transdermal estradiol.
The approved application sites are the lower abdomen, buttock, and upper hip. The patch should go on clean, dry, intact skin. Not the breasts. Not the waistline (clothing friction loosens adhesion). Not an area where you just applied lotion or cream.
Here's why location matters more than most people expect: a clinical pharmacokinetics study comparing buttock versus abdomen application in women wearing the Climara patch found that the buttock delivered a Cmax (peak estradiol concentration) that was 125.1% of the abdomen value, and an AUC (total exposure) that was 117.2% of abdomen (Taggart et al., 2000). In plain terms — the same patch, on your buttock instead of your abdomen, delivers about 17–25% more estradiol.
That's a clinically meaningful difference. If your patch is working but your levels are running higher than expected, it's worth asking where you're placing it.
Be consistent about your application site so your levels stay predictable. If your provider is monitoring your serum estradiol, they should know where you're applying the patch when they interpret your results (Taggart et al., 2000).
Once-Weekly vs. Twice-Weekly: What's the Difference?
The change schedule affects more than just convenience — it changes how stable your estradiol levels are throughout the week.
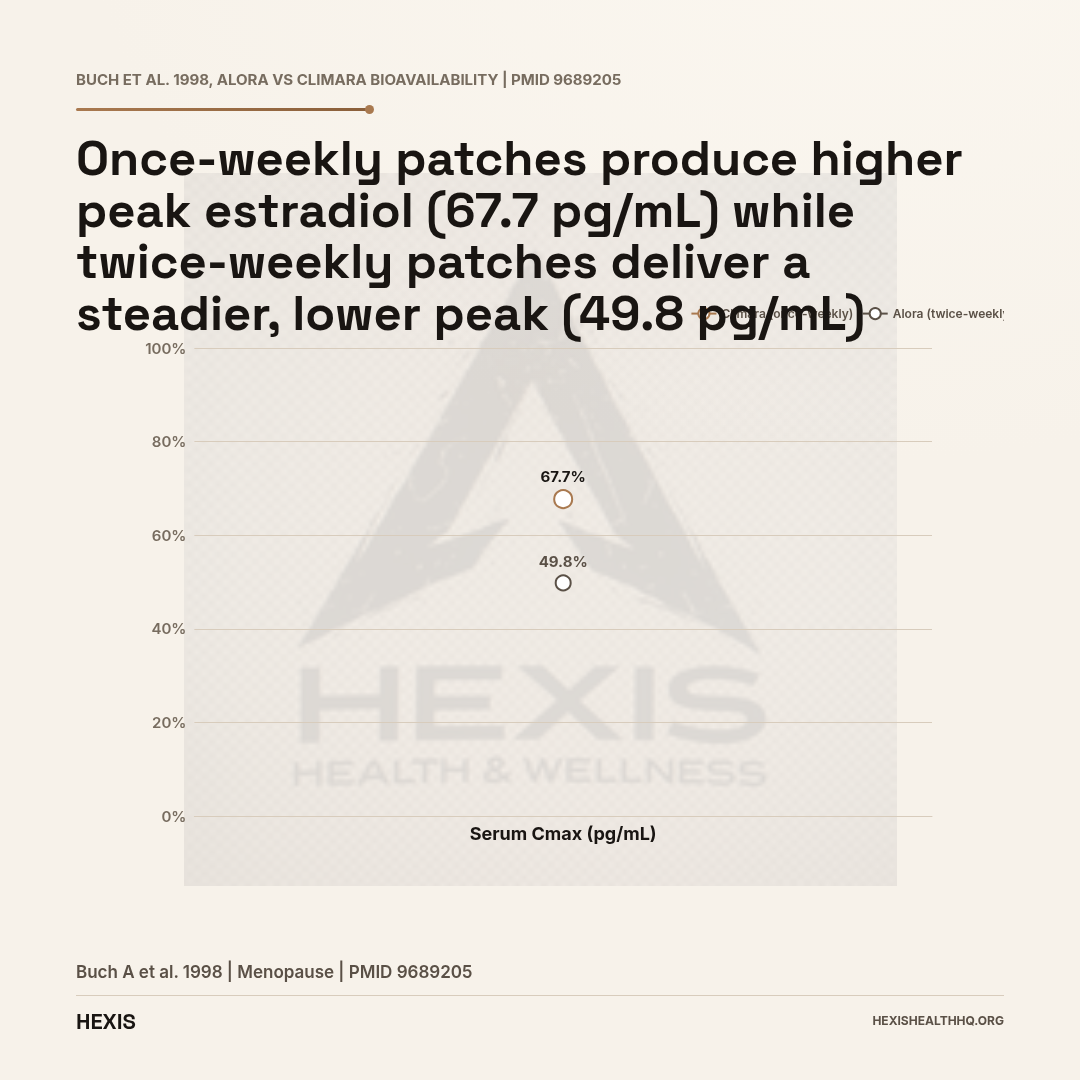
Once-weekly patches (Climara): You change one patch every seven days. Absorption is continuous across the week, but there's a natural decline toward day 6–7 as the reservoir depletes. Serum Cmax with once-weekly Climara was measured at 67.7 pg/mL in a bioavailability comparison study (Buch et al., 1998).
Twice-weekly patches (Vivelle-Dot, Minivelle, Alora): You change the patch every 3–4 days. Because you're refreshing delivery more frequently, the peak-trough fluctuation is smaller. Serum Cmax for twice-weekly Alora was 49.8 pg/mL in the same comparison (Buch et al., 1998) — lower peak, but steadier delivery across the cycle.
Neither is inherently better. Some women do better with once-weekly because of the simpler routine; others prefer twice-weekly because they notice symptoms returning before day seven on a once-weekly patch. This is worth discussing with your provider when choosing your formulation.
Does the Estradiol Patch Cause Blood Clots Like Oral HRT?
The safety question most women ask first — and the one that trips up a lot of providers — is whether the patch raises clot risk the way oral estrogen does. The answer depends entirely on the route of delivery.
Oral estrogens are absorbed through the gut and pass through the liver before entering circulation. That first-pass metabolism causes the liver to upregulate clotting factors, C-reactive protein, and other prothrombotic proteins. This is why oral conjugated equine estrogens (like Premarin) have been associated with increased VTE risk in multiple large studies.
Transdermal estradiol bypasses that first-pass hepatic metabolism entirely. The estradiol goes directly into circulation through your skin, and the liver never sees the bolus. As a result, transdermal estradiol does not raise clotting factors the way oral estrogens do (Conard et al., 1997).
A 2025 systematic review of 23 studies on transdermal drug delivery for menopausal symptoms found that transdermal patches reduce thromboembolism risk by approximately 30% compared to oral HRT — specifically because of the first-pass bypass mechanism (Bostani Khalesi et al., 2025).
The KEEPS trial reinforced this. In 727 recently menopausal women followed for four years, the transdermal estradiol arm saw no cases of venous thrombosis (Miller et al., 2019). Sexual function improved and bone mineral density was maintained — with a safety profile that oral HRT cannot match on the clotting risk dimension.
If you have a history of clotting risk factors but are not in an absolute contraindication category, the transdermal route is the safer conversation to have with your provider. The pill and the patch are not the same thing.
Skin Erythema Rate by Patch Size
Smaller patches produce fewer skin reactions (Ibarra de Palacios et al., 2002)
| Patch | Size | Erythema Rate |
|---|---|---|
What Are the Most Common Side Effects of the Estradiol Patch?
Side effects with the patch tend to be either local — at the application site — or systemic, from estrogen circulating through your body. They're different problems with different fixes.
Local Side Effects
Skin reactions are the most common local issue. These include redness (erythema), itching, and irritation at the application site. The size of the patch matters here: in a direct comparison, the smaller 5 cm² patch (Estradot) produced erythema in 21.4% of users, while the larger 12.5 cm² patch (Climara) produced erythema in 32.3% (Ibarra de Palacios et al., 2002). Smaller patches are easier on the skin.
Site rotation is the main mitigation strategy. Rotating your application site with each change prevents repeated irritation in one area. Some women also find that applying the patch to a slightly different spot each time — a few centimeters away from the previous location — helps.
In the Climara pivotal trial, skin reactions were the primary reason for study withdrawal — a small percentage of participants discontinued due to persistent local irritation (Gordon, 1995). That's not common. But if you're getting significant skin reactions, there are other patch formats (smaller size, different adhesive) worth trying before abandoning transdermal delivery entirely.
Systemic Side Effects
Breast tenderness (mastalgia): This is the most frequently reported systemic side effect. In a randomized comparison of intranasal vs. transdermal estradiol, 15.5% of transdermal users reported moderate-to-severe mastalgia (Lopes et al., 2000). Tenderness is often dose-dependent and may ease after the first few months. If it's significant, your provider may lower your dose or adjust your progestogen.
Breakthrough bleeding and spotting: Common in the first few months, especially if you still have a uterus and are starting progestogen. This usually settles as your body adjusts.
Nausea: Less common with patches than with oral estrogen because you're avoiding the gastrointestinal first pass, but some women still experience it early on.
Headache and mood changes: Some women notice initial mood fluctuations or headaches as estradiol levels stabilize. These tend to resolve within the first 4–8 weeks.
The quality-of-life data from a 2025 randomized controlled trial comparing transdermal estradiol to oral estrogens found that the transdermal group had significantly better scores on menopause-specific quality of life measures — including vasomotor, psychosocial, and physical domains (Tang et al., 2025).
Do You Need Progesterone With the Estradiol Patch?
Women with an intact uterus who use an estradiol patch require progestogen — this is not optional and is not dose-dependent. Estrogen without progestogen causes the uterine lining (endometrium) to thicken with each cycle. Over months and years, that can lead to endometrial hyperplasia and, if untreated, endometrial cancer. Progestogen balances estrogen's proliferative effect on the uterine lining.
The estradiol patch is a systemic estrogen — meaning it circulates throughout your body, including to your uterus. So if you have a uterus, your prescription for a patch should come with a progestogen component (either a separate pill like micronized progesterone, or a combination patch that includes both hormones).
If you've had a hysterectomy, you don't have this requirement. Estrogen-only therapy is standard in that case.
This is a critical point that sometimes gets missed when switching from combination pills to a patch. Make sure your prescriber addresses it explicitly. If you're navigating the broader decision around which form of HRT fits your situation, our article on perimenopause symptoms and treatment explains how estrogen deficiency presents and what different delivery routes target.
The FDA lists absolute contraindications regardless of delivery route: active or prior VTE/arterial thromboembolism, estrogen-dependent cancers, undiagnosed vaginal bleeding, active liver disease, and known or suspected pregnancy. The transdermal advantage is about comparative risk reduction — not elimination. Women with prior clotting events need specialist guidance before starting any systemic estrogen.
Source: FDA prescribing information; Bostani Khalesi et al., 2025
Who Should Not Use an Estradiol Patch?
Certain conditions make systemic estrogen unsafe regardless of delivery route. The FDA lists these as absolute contraindications for the estradiol patch:
- Active or history of venous thromboembolism (DVT, pulmonary embolism) — though transdermal carries lower risk, it is not risk-free in those with a prior VTE without specialist guidance
- Active or history of arterial thromboembolism (stroke, MI)
- Known or suspected estrogen-dependent cancers (breast cancer, certain uterine cancers)
- Undiagnosed abnormal vaginal bleeding
- Active liver disease or a history of estrogen-related liver problems
- Known hypersensitivity to estradiol or patch adhesive components
- Known or suspected pregnancy
This list matters especially because some women hear "lower VTE risk than oral" and assume the patch is safe for everyone. It isn't. The transdermal advantage is about comparative risk — not zero risk. Anyone with a personal or family history of clotting disorders should have a detailed conversation with their provider before starting any form of systemic estrogen.
How Long Before the Patch Works?
Most women notice improvement in hot flashes and night sweats within two to four weeks of starting the estradiol patch. In the Climara pivotal trial, significant reductions in hot flush frequency were measured at week 4, with the full effect apparent by week 11 (Gordon, 1995).
Sleep disruption — which is often driven by night sweats — tends to improve on a similar timeline. Vaginal symptoms (dryness, discomfort) may take longer, sometimes 8–12 weeks, to show full benefit.
The timing hypothesis from the KEEPS trial adds important context: women who started transdermal estradiol within three years of their final menstrual period (the "timing window") showed better outcomes on multiple measures including bone density and sexual function, compared to women who started later (Miller et al., 2019). Earlier initiation appears to matter. If you're reading this while still in perimenopause rather than after your final period, that timing distinction is relevant — our menopause hormone therapy overview breaks down the window-of-opportunity evidence in more detail.
Practical Tips for Getting the Most from Your Patch
Estradiol patch effectiveness depends on correct application, consistent site rotation, and proper disposal — errors in any of these reduce absorption reliability or cause skin reactions. These are the factors that most often explain inconsistent serum levels between lab draws:
Applying the patch correctly:
- Clean skin, fully dry — no lotion, oil, or cream on the area first
- Press firmly with your palm for at least 10–15 seconds
- Check the edges for full contact
- Do not cut the patch to adjust the dose — that disrupts the delivery matrix
Showering and swimming: The patch is designed to stay in place through normal bathing and swimming. If yours repeatedly peels or lifts at the edges, try a different placement site, or ask your provider about a different brand — adhesion varies between formulations (Ibarra de Palacios et al., 2002).
What to do if it falls off: Apply a new patch to a different site and continue your original change schedule. Don't double up to compensate.
Dispose of used patches safely: Used patches still contain active estradiol. Fold the patch in half (sticky side in) and dispose in household trash — not in the toilet, as estradiol is an environmental pollutant.
Climara vs. Vivelle-Dot — Which Is Better?
Neither is universally better. Here's what the data shows:
Climara (once-weekly): Larger patch, single change per week. Produces a higher serum Cmax but more peak-trough variation across the seven-day interval. The larger surface area correlates with slightly higher erythema rates (Ibarra de Palacios et al., 2002). Better for adherence in women who prefer fewer changes.
Vivelle-Dot (twice-weekly): Smaller patch, changed every 3–4 days. Lower Cmax but steadier delivery. The lower erythema rate associated with smaller patches may make it a better fit for women with sensitive skin (Ibarra de Palacios et al., 2002). Some women report fewer end-of-cycle symptom returns because of the more frequent refreshes.
The bioavailability data (Buch et al., 1998) shows these are not equivalent doses — the same labeled mg/day delivers different serum concentrations depending on the formulation. Your provider should check your serum estradiol after starting or switching between brands if symptoms change unexpectedly.
Frequently Asked Questions
Where do you apply an estradiol patch and does location matter?
Apply the patch to the lower abdomen, buttock, or upper hip — on clean, dry, intact skin. Rotate the site with each change. Location matters: the buttock delivers roughly 17–25% more estradiol (Cmax 125.1% vs. abdomen) than the abdomen due to differences in skin thickness and blood flow (Taggart et al., 2000). Keep your site consistent between monitoring visits so your bloodwork is interpretable.
Does the estradiol patch cause blood clots?
Transdermal estradiol carries significantly lower VTE risk than oral estrogens. Because it bypasses first-pass hepatic metabolism, it does not elevate clotting factors the way pills do. A 2025 systematic review found transdermal delivery reduces thromboembolism risk approximately 30% vs. oral HRT (Bostani Khalesi et al., 2025). It is not risk-free for everyone — women with prior VTE need specialist guidance.
What is the starting dose for an estradiol patch?
Most providers start at 0.025–0.05 mg/day and titrate based on symptom response and serum estradiol levels (Sriprasert et al., 2020). The lowest effective dose is the goal. Starting low allows your body to adjust and gives a clear baseline before increasing.
Do I need progesterone with my estradiol patch?
Yes, if you have a uterus. Systemic estrogen without progestogen causes endometrial proliferation that can lead to hyperplasia over time. Progestogen — either as a separate prescription or a combination patch — is required to protect the uterine lining. Women who have had a hysterectomy do not need progestogen.
How long does the estradiol patch take to work for hot flashes?
Most women notice meaningful improvement within two to four weeks. The full effect on hot flush frequency is typically apparent by week 11, as documented in the pivotal Climara trial (n=603) (Gordon, 1995). Night sweats often improve on a similar timeline; vaginal symptoms may take up to 8–12 weeks.
Working With a Provider on HRT
The decision to start an estradiol patch — what strength, what brand, whether you need progestogen, and how to monitor progress — is built around your individual labs and symptom picture. Baseline estradiol levels vary widely between women, and what works for one person's vasomotor symptoms won't necessarily be the right starting point for another.
At HEXIS, we start with labs, not guesswork. In practice, the women who do best on transdermal therapy are the ones whose providers checked a baseline serum estradiol before prescribing — because your starting point determines how far you need to titrate. We see this consistently in clinical practice: a woman who comes in at 8 pg/mL pre-treatment needs a very different starting point than one who comes in at 30 pg/mL. Your provider reviews your full hormone panel, your personal and family history, and your symptoms before building a protocol. If the patch is the right route for you, we'll identify the right dose and check in on your levels as you adjust. Schedule a consultation to start that conversation.
What to Know Before Your Next Appointment
- 1
Patches come in six doses (0.014–0.1 mg/day). Most women start at 0.025–0.05 mg/day and titrate up based on symptoms and labs.
- 2
Where you apply matters. Buttock delivers 17–25% more estradiol than abdomen — tell your provider where you're applying when you get labs.
- 3
The patch does not raise clot risk the way oral estrogen does. It bypasses the liver entirely. A 2025 review found 30% lower VTE risk vs. oral HRT.
- 4
If you have a uterus, you need progestogen alongside your estradiol patch. This is non-negotiable for endometrial protection.
- 5
Skin reactions? Switch to a smaller patch format or rotate sites more aggressively — don't abandon transdermal delivery entirely.