Hormone Replacement Therapy: The Complete Guide (HRT & TRT)
Hormone Replacement Therapy: The Complete Guide (HRT & TRT)
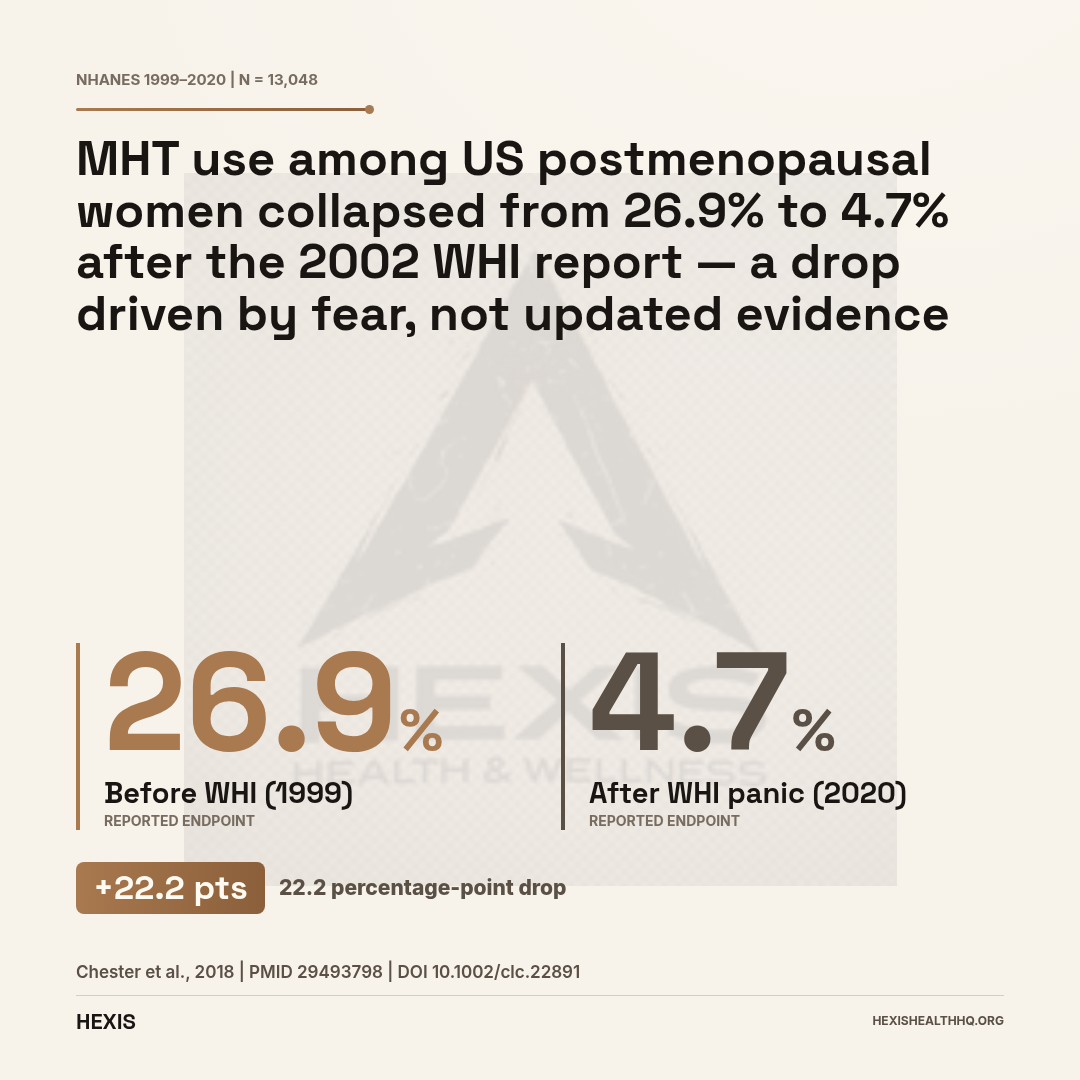
If you've been told that hormone replacement therapy is dangerous, you were given outdated information — and you're not alone. Following a 2002 clinical trial that the press turned into a cancer scare, MHT use among US postmenopausal women collapsed from 26.9% to 4.7% over two decades (Chester et al., 2018). Millions of women who could have benefited stopped, or never started. Twenty-plus years of follow-up data and several major trials later, that picture looks very different.
Quick answer: Hormone replacement therapy (HRT) replaces or supplements hormones the body no longer produces in adequate amounts. For women in perimenopause or menopause, that means estrogen ± progesterone — to relieve symptoms, protect bone density, and reduce long-term cardiovascular and cognitive risk when started at the right time. For men with confirmed low testosterone, it means testosterone replacement therapy (TRT) to restore normal physiological levels. Both have real benefits, real risks, and delivery options that change those risk profiles. Every protocol starts with lab work — not symptoms alone.
What Is Hormone Replacement Therapy?
Hormone replacement therapy is a category of medical treatment that replaces or supplements hormones the body no longer produces at adequate levels — estrogen and progesterone for women in perimenopause or menopause, and testosterone for men with confirmed hypogonadism. It is not a single drug or a single protocol; it looks quite different depending on who is using it and why.
For women going through perimenopause or menopause, HRT (also called menopausal hormone therapy, or MHT) primarily replaces estrogen, with progesterone added for women who still have a uterus. The goal is to relieve symptoms, protect bone density, and — depending on timing and formulation — potentially reduce long-term cardiovascular and cognitive risk (Davis & Baber, 2022).
For men with confirmed low testosterone (hypogonadism), testosterone replacement therapy restores circulating testosterone to a normal physiological range. This addresses symptoms including fatigue, low libido, loss of lean muscle mass, mood changes, and sexual dysfunction.
The overlap is real — both involve hormones, both require lab work and monitoring, and both have been subject to overstated fears and undersold benefits. The mechanisms, populations, and evidence bases are different enough that they deserve separate treatment.
What Did the WHI Actually Find — and What Did Follow-Up Reveal?
The Women's Health Initiative (WHI) is the largest clinical trial ever conducted on female hormone therapy — 27,347 women, two treatment arms, and findings that caused HRT prescriptions to collapse. What the 2002 headlines got wrong, and what 20+ years of follow-up data has clarified, is the single most important thing to understand before making any decision about HRT.
The WHI enrolled women across two arms: conjugated equine estrogen plus medroxyprogesterone acetate (CEE+MPA), and CEE alone for women who had had hysterectomies. The initial combined-arm findings were reported as showing increased breast cancer risk, and the headlines took it from there. Prescriptions dropped. Doctors became reluctant. Women who had been managing their symptoms well were told to stop.
Here's what 20-plus years of additional follow-up has revealed (Chester et al., 2018):
The CEE-alone arm showed the opposite of what people fear. In women without a uterus taking estrogen only, the hazard ratio for breast cancer incidence was 0.78 (95% CI 0.65–0.93) compared to placebo — a 22% reduction in breast cancer risk, not an increase (Chlebowski et al., 2020). The breast cancer signal in the combined arm was tied to the specific progestin used (MPA), not estrogen itself.
The timing of initiation matters enormously — something the original WHI coverage completely missed. Most women in the WHI were started on HRT at age 63 or older, well past the window where estrogen exerts cardiovascular protection. When you look at women who started within 10 years of menopause or under age 60, the risk profile is substantially different (Chester et al., 2018).
This is called the "timing hypothesis," and it's now central to how evidence-based clinicians think about HRT.
Who Is HRT For?
Not every woman going through menopause needs HRT. But many who would benefit have been steered away from it by outdated guidance. Here's who the evidence supports (Davis & Baber, 2022):
Women with significant menopause symptoms. Vasomotor symptoms — hot flashes, night sweats, sleep disruption, brain fog, vaginal dryness, mood changes, joint pain — are all documented consequences of estrogen decline. These are the clearest indication for MHT, and the symptom relief is well-documented.
Women at elevated risk for osteoporosis. MHT reduces fracture risk by 20–40% at all bone sites — and it is one of the only anti-osteoporotic therapies proven effective even in women without pre-existing high fracture risk (Gosset et al., 2021).
Women with early menopause or primary ovarian insufficiency (POI). If menopause hits before age 45 — or before 40, which is POI — the cardiovascular risk is 1.5 to 2-fold higher than women who reach menopause at the typical age (Anagnostis et al., 2019). For these women, MHT to at least the average age of menopause is considered essential, not optional (Sullivan et al., 2016).
Women on the contraindicated list include those with active or recent hormone-sensitive cancers, unexplained vaginal bleeding, or active venous thromboembolism. These require individual evaluation — and "history of breast cancer" is not automatically a contraindication for all HRT types (Kuhle et al., 2016).
Globally, the mean age of natural menopause is 48.8 years (Davis & Baber, 2022). The perimenopause transition — where symptoms often start — can begin years before that last period. Don't wait until menopause is "official" to have the conversation.
Breast Cancer Risk by HRT Type
| HRT Type | Breast Cancer HR | vs. Placebo |
|---|---|---|
Source: Chlebowski et al., 2020; Kotsopoulos et al., 2026
The Benefits of Female HRT: Bones, Brain, and Heart
Bone Protection
MHT reduces fracture risk by 20–40% at all bone sites, including hip, spine, and wrist, across multiple randomized controlled trials (Gosset et al., 2021). It maintains and often increases bone mineral density throughout treatment.
This protection holds regardless of baseline fracture risk. Most other osteoporosis medications are reserved for women already at high risk. MHT is the exception — it works in lower-risk women too.
For women entering menopause early, this benefit comes earlier and matters more. Estrogen decline directly accelerates bone loss, and beginning HRT soon after menopause limits that acceleration.
Cognition and Memory
Timing determines almost everything here — start early and the data is encouraging; start late and it reverses.
A 2024 systematic review and meta-analysis of 34 RCTs enrolling 27,593 women found that among women who underwent surgical menopause, MHT improved global cognition with an effect size of SMD 1.575 (95% CI 0.228–2.921) — a large signal (Andy et al., 2024). For women who started therapy in midlife or close to menopause onset, verbal memory improved with an SMD of 0.394 (95% CI 0.014–0.774).
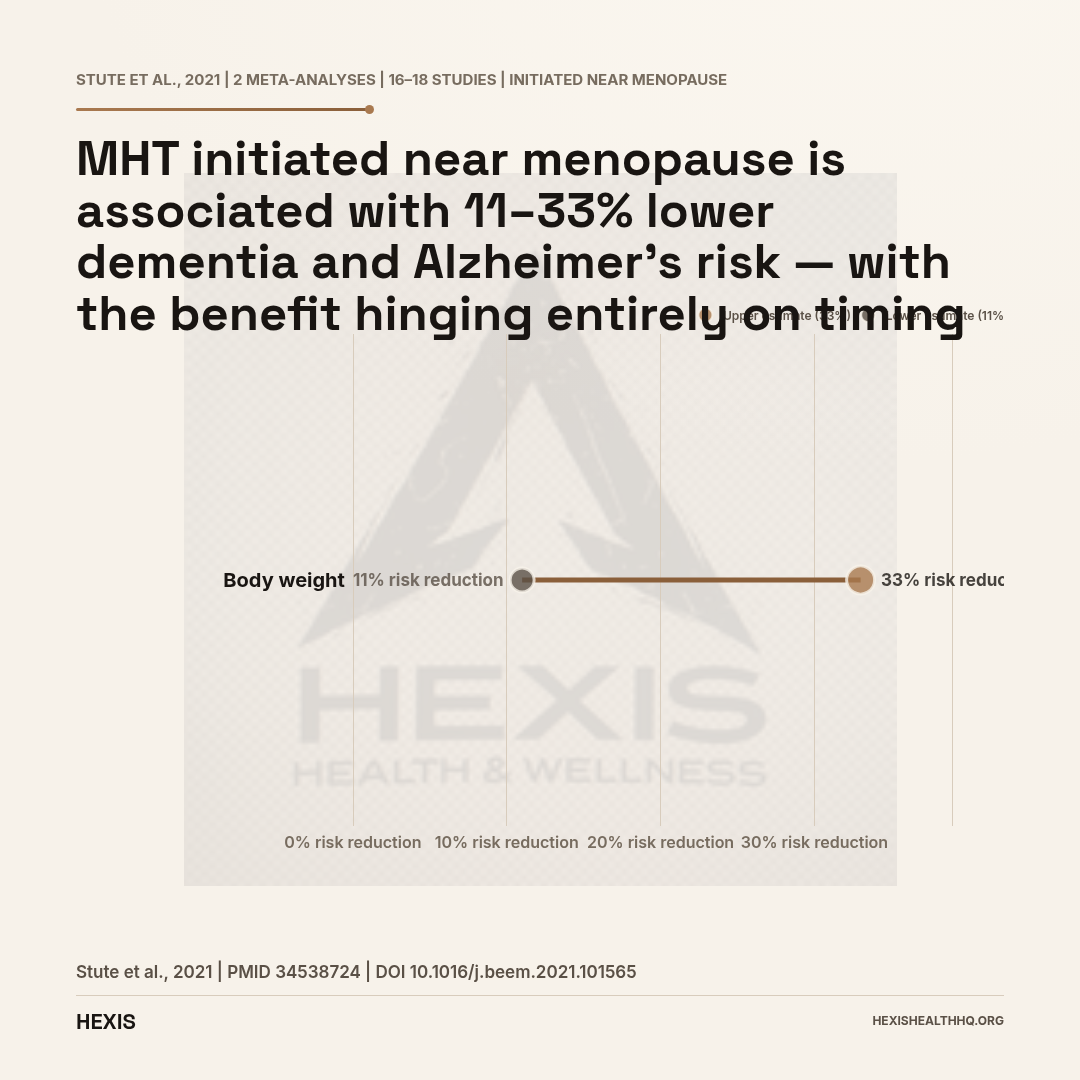
Two meta-analyses covering 16–18 studies found that MHT initiated near menopause is associated with an 11–33% reduction in dementia and Alzheimer's risk (Stute et al., 2021). The KEEPS Continuation Study found no long-term cognitive harm with either oral or transdermal estradiol initiated early (Gleason et al., 2024).
The contrast with the Women's Health Initiative Memory Study (WHIMS) is important: that study found doubled dementia risk with HRT — but those women were all over age 65 when they started therapy. Starting HRT in women aged 65+ who have not used it before is a different clinical situation than initiating at or near menopause.
Cardiovascular Risk
For women who start MHT within 10 years of menopause or before age 60, cardiovascular risk is neutral to modestly favorable. The confusion comes from the WHI, where women were on average 63 years old at enrollment — well outside the protective window.
Women who start late — as most WHI participants did — do not see that benefit. For women with early menopause or POI, the cardiovascular case is even clearer: untreated early menopause carries a 1.5–2-fold increase in cardiovascular disease risk (Anagnostis et al., 2019).
Oral estrogen carries a 1.22–4.50× relative risk increase for blood clots. Transdermal estradiol (patch, gel, spray) bypasses the liver and does not carry this risk — making route of delivery a critical clinical decision for women with elevated VTE risk.
Source: Wu, 2005; Sobel & Shen, 2022
What Are the Risks of HRT?
VTE Risk and How Route Changes It
Oral estrogen carries a measurable VTE risk. Studies show relative risk increases ranging from 1.22 to 4.50-fold compared to non-users for current HRT users (Wu, 2005). Combined estrogen-progestin HRT carries a higher VTE risk than estrogen alone — OR 1.60 (95% CI 1.13–2.26) for the combined form vs. estrogen-only (Wu, 2005).
Transdermal estrogen is different. Because transdermal estradiol bypasses hepatic first-pass metabolism, it does not produce the prothrombotic changes in clotting factors that oral estrogen does. Multiple studies and a scoping review support transdermal estradiol as the preferred route for women at elevated VTE risk (Sobel & Shen, 2022).
Route of delivery changes the risk profile — and it is exactly the kind of detail that gets lost when "HRT" is treated as a single entity.
Breast Cancer Risk by HRT Type
Breast cancer risk from HRT depends entirely on the type — and for some women, the evidence points the other direction entirely.
Estrogen alone (CEE-alone, WHI): Breast cancer incidence HR 0.78 (95% CI 0.65–0.93) vs. placebo in women without a uterus — protective, not harmful (Chlebowski et al., 2020).
Combined CEE+MPA: Modestly increased risk, tied to the specific progestin (MPA) used. Micronized progesterone appears to carry a more favorable breast cancer risk profile than synthetic progestins (Armeni et al., 2021).
BRCA1/2 carriers post-oophorectomy: Estrogen-alone HRT was associated with a breast cancer HR of 0.37 (95% CI 0.24–0.57, n=1,352, mean 5.6 years follow-up) — a 63% reduction vs. untreated controls (Kotsopoulos et al., 2026). This directly counters the widespread assumption that BRCA carriers cannot safely use HRT.
The overall risk from combined HRT is real but contextual. For most women with significant symptoms or early menopause, the benefit-to-risk ratio tips toward treatment.
For a deeper look at estrogen formulations, see our guide to estradiol patches and how Premarin compares to bioidentical options.
Delivery Methods: Why Route Matters
The route estrogen takes into your body changes its biological effects in clinically meaningful ways — oral estrogen raises VTE risk up to 4.5-fold through hepatic first-pass metabolism, while transdermal formulations (patch, gel, spray) bypass the liver entirely and do not carry this risk. Beyond clotting, route also affects lipids, blood pressure, and convenience.
| Route | Examples | VTE Risk | Notes |
|---|---|---|---|
| Oral tablet | Estrace, Premarin | Elevated (first-pass effect) | Convenient; raises HDL |
| Transdermal patch | Vivelle-Dot, Climara | No increase | Steady levels; preferred for VTE risk |
| Transdermal gel | EstroGel, Divigel | No increase | Flexible dosing; skin transfer risk |
| Transdermal spray | Evamist | No increase | Quick-dry; similar to gel |
| Vaginal ring | Estring, Femring | Minimal | Local or systemic depending on type |
| Subcutaneous pellet | Compounded | No increase | Long-acting; compounded only |
For women with a uterus, a progestogen is added to protect the endometrium. Micronized progesterone (Prometrium) is bioidentical and appears to carry a more favorable breast and cardiovascular profile than MPA (Lundberg et al., 2020).
"Bioidentical" is not a regulatory category in the US — but FDA-approved bioidentical products exist. Compounded bioidentical HRT lacks the same evidence base and regulatory oversight as approved products; the claims made about custom compounding often exceed the available evidence (Stuenkel, 2021).
The preference for bioidentical estradiol plus micronized progesterone over CEE+MPA is supported by the evidence on VTE risk, breast risk, and cardiovascular profile (Armeni et al., 2021).
For a full look at delivery options for menopause specifically, see our guide to HRT for menopause.
Male TRT: When Low Testosterone Needs Treatment
Testosterone replacement therapy is indicated when a man has both confirmed low testosterone (morning serum levels consistently below 300 ng/dL on at least two separate draws) and clinical symptoms — fatigue, low libido, loss of lean mass, mood changes, or cognitive difficulties. The lab number alone is not enough, and symptoms alone are not enough. Both together define clinical hypogonadism.
Symptoms of low testosterone typically include:
- Persistent fatigue and low energy
- Decreased libido and sexual function
- Loss of lean muscle mass and increased body fat
- Mood changes, irritability, or depression
- Cognitive difficulties and poor concentration
If your doctor ran a single testosterone test in the afternoon and told you it was "fine," the protocol was not right. Testosterone follows a diurnal rhythm — levels are highest in the morning (typically 7–10 AM) and decline through the day. A single afternoon draw can miss true hypogonadism.
For a full breakdown of what low testosterone looks like and how it is confirmed, see our article on low testosterone symptoms.
TRT Benefits: Body Composition, Sexual Function, and Bone Density
Testosterone replacement therapy in men with confirmed hypogonadism improves body composition, sexual function, bone density, and mood — with the magnitude of benefit correlating with the degree of deficiency at baseline. Men with the lowest pretreatment testosterone levels consistently show the largest gains across all four domains (Lincoff et al., 2023).
Body composition. TRT increases lean muscle mass and reduces fat mass, particularly in the visceral (abdominal) compartment. This happens through testosterone's direct anabolic effects on muscle protein synthesis and its role in reducing the conversion of testosterone to estrogen in fat tissue.
Sexual function. Libido and erectile function respond to TRT, though erectile dysfunction with a purely vascular cause may also require additional treatment. These are often the symptoms that bring men in — and often the first to improve.
Bone density. Like estrogen in women, testosterone is an important determinant of bone mineral density in men. Hypogonadism significantly increases fracture risk, and TRT can reverse that.
Mood and cognitive function. Men with confirmed hypogonadism frequently report improved mood, motivation, and mental clarity on TRT. The brain fog lifts. That matters as much as the physical changes, and it is often what patients report first at their 3-month follow-up.
Is TRT Safe for the Heart?
The TRAVERSE trial gave TRT its definitive cardiovascular safety answer — in the hardest possible population to test.
TRAVERSE enrolled 5,204 men with confirmed hypogonadism and elevated cardiovascular risk and randomized them to testosterone therapy or placebo for approximately 4 years. The primary endpoint was major adverse cardiovascular events (MACE).
The result: TRT was non-inferior to placebo for MACE (Lincoff et al., 2023). In the highest-risk men — those with pre-existing cardiovascular disease — TRT did not increase the rate of heart attacks, strokes, or cardiovascular death.
Polycythemia (elevated hematocrit) and atrial fibrillation occurred at slightly higher rates in the TRT arm, which is why monitoring hematocrit is part of standard TRT management. That is not a reason to avoid TRT in appropriate candidates — it is a reason to monitor it.
For the full picture on injectable testosterone protocols, see our article on injectable testosterone.
TRT Delivery Methods
Testosterone replacement therapy is available in seven delivery forms — injections, gels, patches, pellets, buccal, oral, and nasal — each with distinct pharmacokinetics, dosing frequency, and practical tradeoffs. The method chosen affects both convenience and how consistently testosterone levels are maintained.
| Method | Examples | Frequency | Notes |
|---|---|---|---|
| Injection (IM or SubQ) | Testosterone cypionate, enanthate | Weekly to biweekly | Most common; cost-effective |
| Topical gel | AndroGel, Testim | Daily | Convenient; transfer risk to partners |
| Transdermal patch | Androderm | Daily | Consistent levels; skin reactions |
| Subcutaneous pellet | Testopel | Every 3–6 months | Long-acting; minor procedure |
| Buccal | Striant | Twice daily | Uncommon; gum placement |
| Oral | Jatenzo | Twice daily | Newer; hepatic metabolism |
| Nasal | Natesto | Three times daily | Short-acting; no suppression |
Weekly subcutaneous injections of testosterone cypionate have become one of the more popular approaches in clinical TRT practice — steady levels, patient control, cost-effective.
Testosterone for Women: An Overlooked Area
No FDA-approved testosterone product for women exists in the US — but that reflects a regulatory gap, not an evidence gap. Off-label testosterone is endorsed for hypoactive sexual desire disorder (HSDD) in postmenopausal women by the International Society for the Study of Women's Sexual Health (ISSWSH), the Endocrine Society, and the British Menopause Society, based on multiple randomized controlled trials showing consistent benefit.
The absence of an approved product reflects historical underfunding of women's sexual health research, not a safety concern. Testosterone can be prescribed off-label by a physician using compounded preparations or male products at lower doses. Labs, starting low, and titrating up are the standard approach.
TRT and Drug-Tested Sports
If you compete in drug-tested sports, testosterone is prohibited under WADA's S1 Anabolic Agents category. A Therapeutic Use Exemption (TUE) is available for men with confirmed hypogonadism, but it requires documentation and pre-approval. Estrogen manipulation for women falls under S4 prohibitions.
HEXIS works with athletic patients on the documentation side — but TUEs are granted by governing bodies, not providers.
Monitoring After Starting HRT or TRT
Starting HRT or TRT isn't a set-and-forget prescription. Ongoing monitoring is what separates a safe protocol from a guess.
For women on MHT:
- Annual mammogram (standard screening — not an HRT-specific requirement for most women)
- Bone density scan at baseline and periodic follow-up
- Symptom review and dose adjustment as needed
- Blood pressure check for oral estrogen users
- Endometrial monitoring (ultrasound or biopsy) if breakthrough bleeding occurs
For men on TRT:
- Testosterone levels (total and free) at 3 months after initiation, then annually
- Hematocrit (to watch for polycythemia — the main safety metric from TRAVERSE)
- PSA (prostate-specific antigen) — TRT does not cause prostate cancer, but it can accelerate existing disease
- Lipid panel
- Estradiol if symptoms suggest conversion issues
- Testicular volume if fertility preservation is a concern
Bioidentical HRT: What the Term Actually Means
"Bioidentical" hormones are molecules structurally identical to the hormones your body produces — as opposed to synthetic analogs or animal-derived hormones. Estradiol (not CEE) is bioidentical. Micronized progesterone (Prometrium) is bioidentical.
FDA-approved bioidentical products exist and have the same evidence base as conventional HRT. The category is not synonymous with "compounded" or "custom-mixed." When people talk about "bioidentical HRT" from a compounding pharmacy, they're referring to a different product with less regulatory oversight — not necessarily a safer or better-evidenced one (Stuenkel, 2021).
Frequently Asked Questions
Is hormone replacement therapy safe?
For most women under 60 who start within 10 years of menopause, the benefit-to-risk ratio for HRT is favorable. The 2002 WHI findings that drove widespread fear applied specifically to older women using oral CEE+MPA — not to the broader population who now considers HRT. Route, formulation, timing, and individual health history all matter (Chester et al., 2018).
Does HRT cause breast cancer?
It depends on the type. Estrogen-alone HRT (in women without a uterus) was protective in the WHI 20-year follow-up — HR 0.78 vs. placebo (Chlebowski et al., 2020). Combined estrogen-progestin with MPA showed a modest increase. Estrogen-alone in BRCA1/2 carriers post-oophorectomy showed a 63% reduction in breast cancer risk — HR 0.37 (Kotsopoulos et al., 2026). This is not a simple yes or no.
Does testosterone therapy increase heart attack risk?
No — not in appropriately selected men with hypogonadism. The TRAVERSE trial (n=5,204, 4 years) found TRT non-inferior to placebo for major adverse cardiovascular events, including in men with pre-existing cardiovascular disease (Lincoff et al., 2023). Hematocrit monitoring is required; polycythemia is the main cardiac-adjacent risk.
Which delivery method is safest for blood clots?
Transdermal estradiol — patch, gel, spray — does not carry the same VTE risk as oral estrogen because it bypasses hepatic first-pass metabolism. For women with elevated VTE risk, transdermal is the recommended route (Sobel & Shen, 2022).
Can I use HRT with a BRCA gene mutation?
If you have had a risk-reducing oophorectomy, estrogen-alone HRT appears to reduce breast cancer risk — HR 0.37 (95% CI 0.24–0.57) compared to untreated women (Kotsopoulos et al., 2026). This finding from a 2026 study of 1,352 BRCA carriers directly challenges the common assumption. Individual evaluation with a specialist is essential.
Working With a Provider
HRT and TRT are not self-prescribing categories. Every evidence-based protocol starts with labs — not symptoms alone, not guesswork. At HEXIS, the workup for either female HRT or male TRT includes a full hormone panel, metabolic markers, and a clinical evaluation before any prescription is written.
On the men's side: a new patient comes in with fatigue and a testosterone result that says "normal." The actual number is 310 ng/dL — technically in range, but in the bottom 10% of the reference range for a 42-year-old. Symptoms are consistent. We draw a second morning sample, check free testosterone and SHBG, rule out secondary causes. That's when the clinical picture becomes clear enough to act on.
On the women's side: a 48-year-old presents with 18 months of disrupted sleep, brain fog, and joint pain that started "out of nowhere." Her primary care doctor offered antidepressants. At HEXIS, the full picture — FSH, estradiol, symptom timeline — makes the perimenopause transition obvious. She starts transdermal estradiol, and at the 8-week check, the sleep and cognitive symptoms are largely resolved. She'd been three months from being put on an SSRI she didn't need.
If you're experiencing symptoms that suggest hormone decline — whether that's menopausal symptoms, persistent fatigue, or changes in body composition and libido — the conversation starts with data.
Medically reviewed by the HEXIS Health Medical Team — board-certified physicians specializing in hormone optimization, metabolic health, and performance medicine. Citations reflect peer-reviewed evidence from JAMA, NEJM, and Nature Reviews Endocrinology. Content is updated as clinical trial data evolves.
Schedule a consultation to have your labs reviewed and discuss whether HRT or TRT is appropriate for your situation.
- 1
Estrogen-alone HRT reduces breast cancer risk by 22% in women without a uterus — opposite of the 2002 headlines
- 2
Transdermal estrogen avoids the VTE risk of oral estrogen entirely — route matters as much as formulation
- 3
TRAVERSE (n=5,204) confirmed TRT is cardiovascular-safe in men with hypogonadism, even with pre-existing heart disease
- 4
Timing is everything: HRT initiated within 10 years of menopause or before age 60 has a fundamentally different risk profile than late initiation
- 5
Every protocol starts with labs — not symptoms alone, not guesswork