Low Testosterone Symptoms in Men: What the Research Actually Shows
Low Testosterone Symptoms in Men: What the Research Actually Shows
Most men who have low testosterone don't know it. They think they're just tired. Stressed. Getting older. Their doctor ran labs, said everything looked "normal," and sent them home. But fatigue, low libido, mood changes, and muscle loss that won't quit aren't just life — they're the core cluster of low testosterone symptoms in men, and they're recognizable, measurable, and in many cases treatable.
Here's what the actual evidence says about what's happening in your body, who gets it, and how it's properly diagnosed.
The short answer: Low testosterone (below 300 ng/dL on two morning measurements) causes a recognizable set of symptoms — reduced libido, fatigue, mood changes, muscle loss, and erectile dysfunction. The TRAVERSE trial (n=5,204), the largest randomized trial ever conducted on testosterone therapy, confirmed these symptom clusters in hypogonadal men and showed that testosterone replacement therapy improved sexual function and mood versus placebo. Diagnosis requires both symptoms and biochemical confirmation — symptoms alone are not sufficient for treatment.
What Is Low Testosterone — and What Count as "Low"?
Your testosterone level isn't just a number. The Endocrine Society's clinical practice guideline defines hypogonadism as a total testosterone level below 300 ng/dL on two separate morning measurements, in a man who also has symptoms (Bhasin et al., 2010). That last part matters. Neither finding alone is enough to diagnose or treat. You need both.
Why morning? Testosterone peaks between 7 and 10 AM. A measurement at 3 PM can look artificially low even in men with completely normal hormone production. One afternoon result tells you almost nothing.
The 300 ng/dL threshold sounds clear-cut, but many men feel the effects starting higher. That's partly why symptoms matter as much as the number. The Endocrine Society guideline puts it plainly: androgen deficiency is a clinical syndrome — it's defined by the combination of signs, symptoms, and biochemical evidence, not a single lab value.
If you're trying to understand whether treatment makes sense, our overview of testosterone replacement therapy covers the options and what to expect from the process.
There are two main types of hypogonadism:
- Primary hypogonadism — the testicles don't produce enough testosterone (causes include Klinefelter syndrome, injury, chemotherapy, orchitis)
- Secondary hypogonadism — the pituitary or hypothalamus fails to signal the testicles properly (causes include pituitary tumors, obesity, opioid use, and sometimes idiopathic)
The EAA (European Academy of Andrology) guidelines further distinguish functional hypogonadism — low testosterone that results from reversible conditions like obesity, metabolic syndrome, or chronic illness — from organic, structural causes (Huhtaniemi et al., 2020). Why does that distinction matter? Because if weight loss or treating sleep apnea can normalize your levels, that may be worth trying before starting TRT.
How Common Is Low Testosterone?
If you're in your 30s, it's probably not that common. If you're in your 60s, it's not rare.
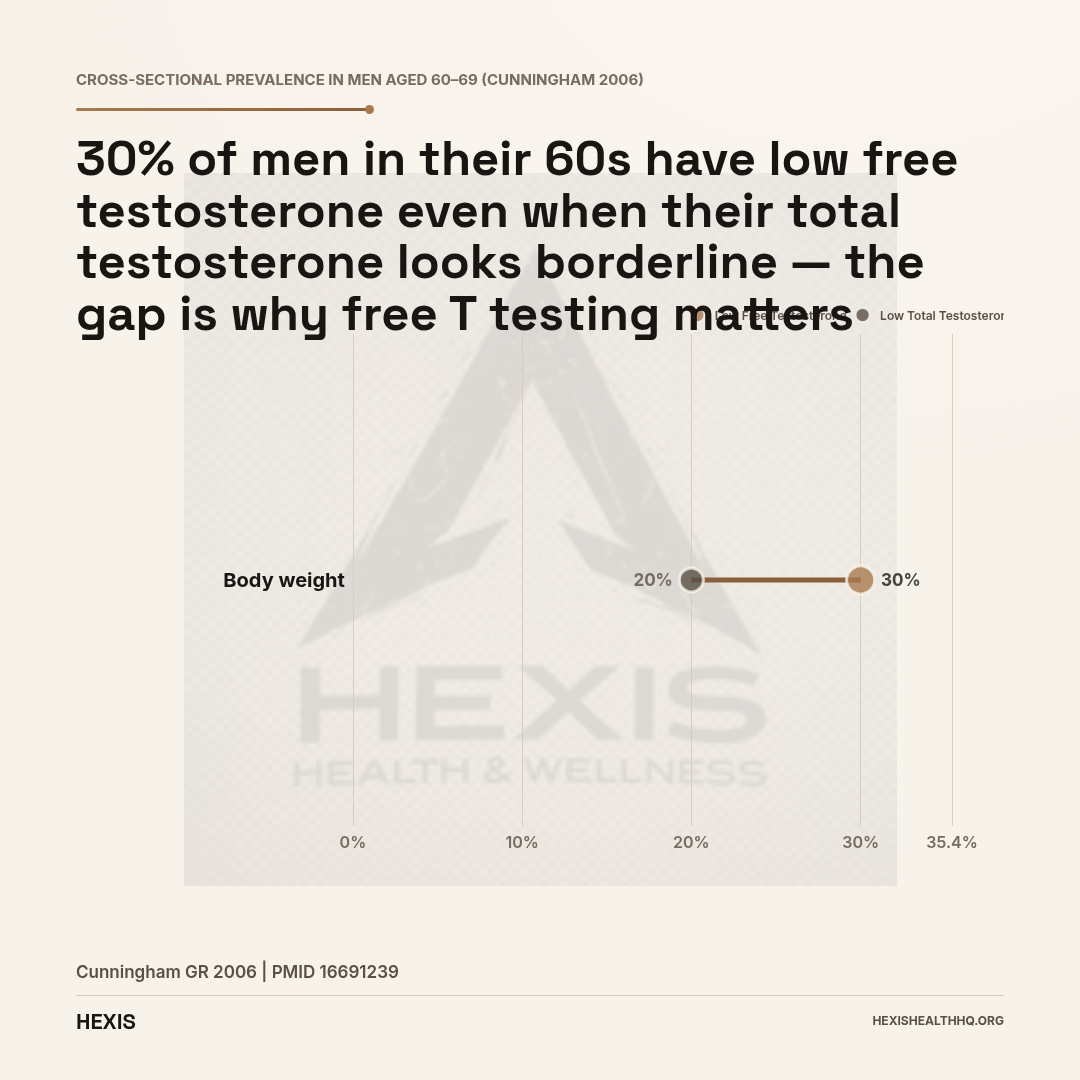
Testosterone declines at roughly 1–2% per year after age 40 (Wu et al., 2010). That's slow enough that most men don't notice it happening — until they do. By the time a man reaches his 60s, approximately 20% have low total testosterone. About 30% of men in that same age range have low free testosterone, which is the biologically active fraction your cells actually use (Cunningham, 2006). By age 80, more than half of men qualify as hypogonadal.
But age isn't the only driver. Obesity, type 2 diabetes, sleep apnea, chronic opioid use, and metabolic syndrome all suppress testosterone — often substantially. Men who are obese have lower levels of sex hormone-binding globulin (SHBG), which means more testosterone gets converted into estrogen in fat tissue, further dropping the amount available to your cells.
The result: two men the same age can have wildly different testosterone levels depending on their metabolic health, and the man with more fat and less sleep is almost certainly lower.
The Five Symptom Clusters You Need to Know
The research consistently groups low testosterone symptoms into five distinct domains. Understanding them this way matters — because "I'm tired" means something different when you also have low libido and you've lost 10 pounds of muscle in two years.
Sexual Symptoms — The Most Documented
Sexual symptoms are the best-studied and most clinically specific cluster. The two most common are reduced libido (sexual desire) and erectile dysfunction.
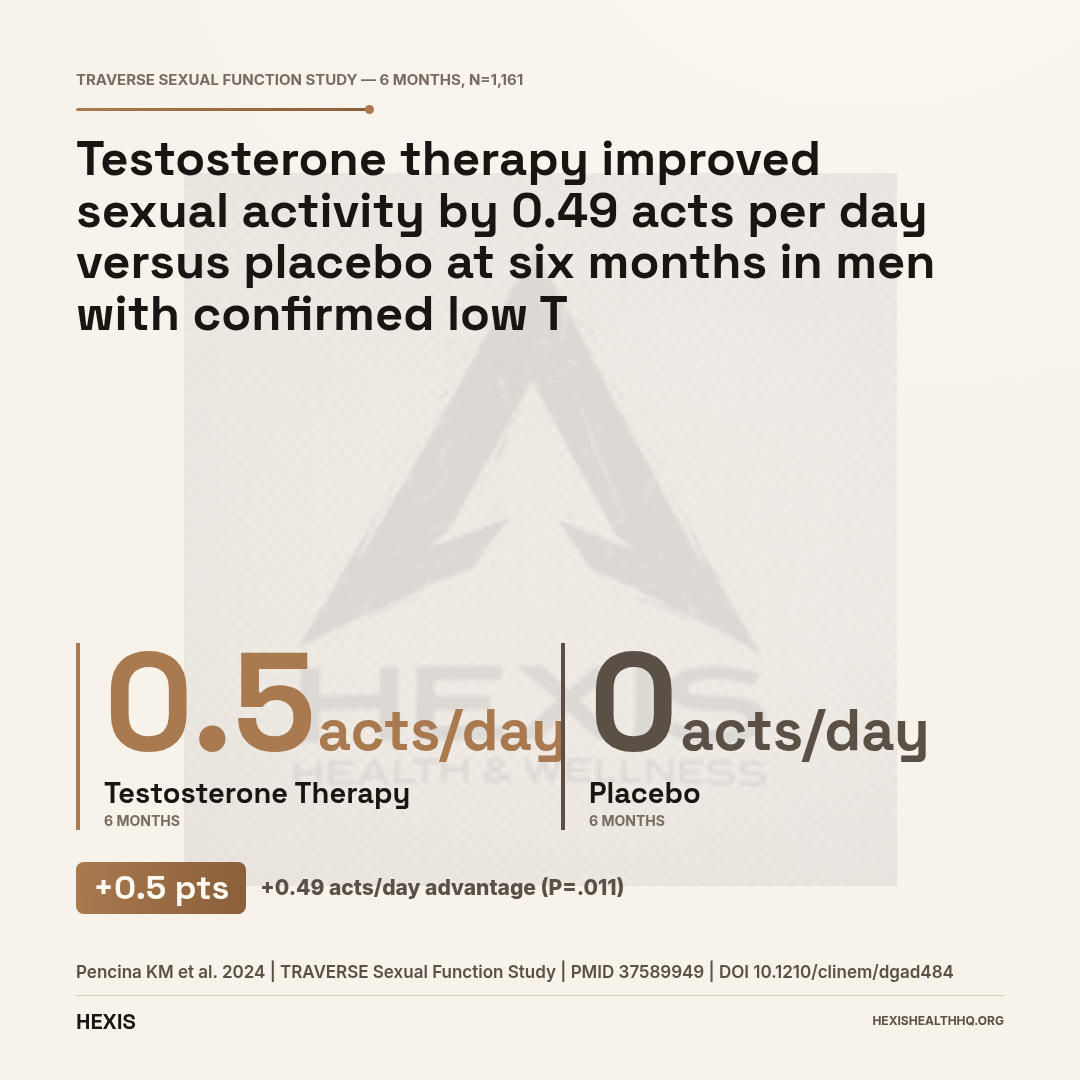
The TRAVERSE Sexual Function Study enrolled 1,161 men from the larger 5,204-person trial who had low libido plus confirmed low testosterone (Pencina et al., 2024). At six months, men on testosterone replacement therapy (1.62% testosterone gel) reported 0.49 more sexual acts per day compared to the placebo group — a statistically significant difference (95% CI [0.19, 0.79]; P=.011). That held at 12 months as well.
Sexual desire impairment is the most consistently testosterone-linked symptom across the research. The EAA guidelines estimate that testosterone needs to fall below approximately 8 nmol/L (about 231 ng/dL) before libido reliably decreases (Huhtaniemi et al., 2020). Erectile dysfunction has a more complicated relationship with testosterone — it's strongly linked in men with frank hypogonadism, but ED in men with borderline or low-normal levels is often driven by other factors (vascular disease, diabetes, performance anxiety). As one major review put it: TRT reliably improves ED in men with overt hypogonadism, but it's not a universal fix for every man who has difficulty getting erections (Rastrelli & Maggi, 2018).
The practical takeaway: if your libido has dropped noticeably and your levels are confirmed low, there's strong evidence TRT can help. If your only complaint is ED, get a cardiovascular workup too — and read more about how erectile dysfunction connects to hormonal health.
Energy and Vitality — Real but Non-Specific
Persistent fatigue, low motivation, and that particular fog where you're trying to think clearly and can't quite get there — these are genuine low T symptoms. They're also the least specific ones.
Fatigue and brain fog appear in thyroid disorders, sleep apnea, depression, anemia, and dozens of other conditions. That doesn't mean testosterone isn't contributing. The TRAVERSE trial showed modest but statistically significant improvements in energy and vitality in men receiving TRT versus placebo (Bhasin et al., 2024). But "modest" is the honest word — testosterone isn't a cure-all for fatigue.
What this means practically: if fatigue is your only symptom and your testosterone comes back at 295 ng/dL, the picture is more complicated than it looks. If fatigue is stacked on top of low libido, muscle loss, and low mood, that cluster tells a clearer story.
Body Composition — The Slow Creep
Men with hypogonadism tend to lose muscle and gain fat — particularly visceral (belly) fat. This happens slowly and gets attributed to aging, stress, or diet. Sometimes it's all three. But testosterone has direct effects on muscle protein synthesis and fat cell metabolism, so genuinely low levels will shift body composition even in men who are exercising.
The Endocrine Society guideline flags decreased lean muscle mass and increased adiposity as recognized features of androgen deficiency (Bhasin et al., 2010). Multiple clinical trials have shown TRT improves lean mass and reduces fat mass in hypogonadal men, though effect sizes in older men with functional hypogonadism are more modest than in younger men with primary hypogonadism.
There's a feedback loop here worth knowing: obesity itself suppresses testosterone. More fat means more aromatase activity, which converts testosterone to estrogen. More estrogen means more fat storage. Breaking that cycle sometimes requires treating both sides — addressing metabolic health and confirming whether hormonal correction is needed.
Mood — The Symptom Most Men Don't Connect
Here's a statistic that should get more attention: in the TRAVERSE trial, 50.8% of the 5,204 enrolled hypogonadal men had significant depressive symptoms at baseline, measured by PHQ-9 scores above 4 (Bhasin et al., 2024). Half. That's not a coincidence — it's a pattern.
Testosterone plays a recognized role in mood regulation, self-confidence, and sense of well-being. Low levels are associated with dysthymia, fatigue, inertia, reduced motivation, and anxiety — not just low libido (Zitzmann, 2020). And these symptoms often get treated as depression in isolation, without anyone checking testosterone.
The TRAVERSE depression substudy found that TRT produced modest but statistically significant improvements in mood versus placebo. That aligns with clinical experience: many men on TRT report that the mood improvement was more meaningful to them than the libido improvement.
None of this means testosterone is an antidepressant. Clinical depression needs proper evaluation. But if a man has depression and confirmed hypogonadism and hasn't had his testosterone levels addressed, treating only one is incomplete. For more on the mood and energy side of hormone optimization, see our article on HRT benefits and risks.
Physical Signs — The Ones Most People Miss
These get overlooked because they look like other things:
- Decreased bone density — testosterone is essential for maintaining bone mineral density. Hypogonadal men have higher rates of osteopenia and osteoporosis. This is often discovered only after a fracture.
- Anemia — testosterone stimulates erythropoiesis (red blood cell production). Low T can cause a mild normocytic anemia that doesn't respond to iron supplementation.
- Reduced body and facial hair — a slow decrease in beard growth or body hair is sometimes the first sign men notice
- Gynecomastia — breast tissue enlargement, resulting from the shift in testosterone-to-estrogen ratio
- Reduced testicular volume — a clinical sign that appears with longer-term hypogonadism
- Hot flashes and night sweats — vasomotor symptoms that most people associate with menopause but can occur in men with severely low testosterone
Wu et al. (2010) in their landmark NEJM study of late-onset hypogonadism identified bone density loss, anemia, and fatigue alongside sexual symptoms as the core clinical features — noting that the non-sexual symptoms are consistently under-recognized.
What Does "Low T" Feel Like Day to Day?
Low testosterone symptoms in daily life are often vague enough to go unrecognized for years — fatigue, flat mood, reduced drive, and declining gym performance are each easy to attribute to stress or aging rather than a hormone problem (Khera et al., 2016). That's why the average man with hypogonadism is diagnosed late, if at all.
There's a reason men often don't bring this up with their doctor: the symptoms feel like they belong to other diagnoses, or to nothing in particular.
You're not sleeping as well. You go to the gym but the gains aren't there anymore. You snap at your partner more. You can go a week without thinking about sex and it doesn't really bother you — but you vaguely remember when it would have. Your morning motivation, the drive you used to have to just do things, is quieter. You're not depressed exactly. You're just flat.
That emotional flatness — the blunting of motivation, drive, and well-being — is one of the most commonly described experiences among hypogonadal men, and one of the least often attributed to testosterone until something changes it.
Can Low Testosterone Cause Depression and Anxiety?
This is worth addressing directly because it's one of the most searched questions — and because the answer carries clinical weight.
The TRAVERSE depression data showed that 50.8% of hypogonadal men had clinically significant depressive symptoms at baseline, and TRT produced meaningful improvements versus placebo (Bhasin et al., 2024). Testosterone acts on brain regions involved in mood regulation. Low levels are associated with increased rates of anxiety, depression, and emotional instability in population studies.
But the relationship runs both ways: depression also suppresses testosterone, via cortisol and hypothalamic-pituitary signaling. Untreated depression can lower testosterone, and low testosterone can drive depressive symptoms. They feed each other.
The key clinical point: if you're being treated for depression and not responding well, and your testosterone has never been measured, that's a gap worth closing. It doesn't mean testosterone is the cause. But ordering the test takes one morning blood draw — and the answer changes the differential either way.
Total vs. Free Testosterone
| Total Testosterone | Free Testosterone | |
|---|---|---|
| What it measures | ||
| Share of total | ||
| Diagnostic threshold | ||
| Who needs free T tested | ||
| SHBG impact |
What Is the Difference Between Total and Free Testosterone?
Your lab report shows two numbers (sometimes more). Here's what they mean.
Total testosterone is everything in your blood — testosterone bound to SHBG (sex hormone-binding globulin), testosterone bound loosely to albumin, and free testosterone. The 300 ng/dL diagnostic threshold applies to total testosterone.
Free testosterone is the fraction not bound to any protein — what's actually available to enter cells and do things. It represents about 1–3% of total testosterone in most men.
Why does the distinction matter? Because SHBG varies. Men who are obese or insulin resistant tend to have lower SHBG, which means more free testosterone relative to total. Older men and men with hyperthyroidism tend to have higher SHBG, meaning their free testosterone is a smaller proportion of total. A man with a total testosterone of 320 ng/dL and low SHBG might have normal free T and no symptoms. A man with a total of 380 ng/dL and high SHBG might have genuinely deficient free T and feel every symptom.
This is why the Endocrine Society and EAA guidelines recommend measuring free testosterone (calculated or direct) when total T is borderline, or when SHBG abnormalities are suspected — which includes obesity, older age, liver disease, and thyroid conditions (Bhasin et al., 2010; Huhtaniemi et al., 2020).
Symptoms alone are not sufficient for diagnosis
The FDA's 2015 labeling update requires that low testosterone diagnosis be confirmed by both symptoms AND two separate morning blood tests below 300 ng/dL. Testing once — or treating based on symptoms without labs — does not meet the clinical standard.
Source: FDA 2015 testosterone labeling guidance; Endocrine Society guideline (Bhasin et al., 2010 — PMID 20525905)
How Is Low Testosterone Diagnosed?
The Endocrine Society guideline is explicit: diagnosis requires both symptoms and two separate morning testosterone measurements below 300 ng/dL (Bhasin et al., 2010). One measurement is not sufficient, because testosterone levels vary day to day.
The steps:
- Symptom assessment — using validated tools like the Aging Males' Symptoms (AMS) scale or clinical interview to document the presence and severity of hypogonadal symptoms
- Two morning blood draws (7–10 AM), on different days, measuring total testosterone
- Free testosterone measurement when total T is borderline (270–400 ng/dL range) or SHBG is suspected to be abnormal
- LH and FSH to distinguish primary from secondary hypogonadism
- Rule out reversible causes — sleep apnea, obesity, opioid use, hyperprolactinemia
The FDA's 2015 labeling update reinforced this: testosterone is approved only for hypogonadism confirmed by both symptoms AND low morning testosterone — not for age-related testosterone decline alone. The FDA's concern was that "low T" was being treated as a normal aging condition without adequate biochemical confirmation — which isn't supported by evidence and carries real treatment risks.
The TRAVERSE trial (NCT03518034) required all 5,204 participants to meet exactly this standard: at least one hypogonadal symptom plus confirmed testosterone below 300 ng/dL on two measurements, in men aged 45–80 with cardiovascular disease or elevated CVD risk (Bhasin et al., 2023). That's the standard. Meeting it matters.
Does Low Testosterone Cause Weight Gain?
The relationship between testosterone and body weight goes in both directions — and understanding that bidirectionality changes how you think about treatment.
Low testosterone promotes fat storage, particularly visceral (abdominal) fat, and reduces the body's ability to build and maintain muscle. Less muscle means lower resting metabolic rate, which makes weight gain easier and weight loss harder. This is a real, documented biological mechanism.
But here's the other direction: fat tissue contains aromatase, the enzyme that converts testosterone to estrogen. The more fat a man carries, the more testosterone he converts — which further drops his levels. Obesity also suppresses LH (the pituitary signal to make testosterone), creating secondary hypogonadism through a metabolic pathway.
This means that in some men, meaningful weight loss can significantly raise testosterone levels on its own — without TRT. The EAA guidelines note this explicitly: for men with functional hypogonadism, treating the underlying cause (losing weight, treating sleep apnea) may normalize levels (Huhtaniemi et al., 2020). That doesn't make TRT the wrong choice, but it does change what the first step looks like in some cases.
What About Athletes and WADA Prohibition?
Testosterone is prohibited in competitive sport under WADA's S1 Anabolic Agents category — banned at all times, including out-of-competition periods. Athletes with documented hypogonadism can apply for a Therapeutic Use Exemption (TUE) from USADA, but the exemption requires formal biochemical diagnosis and medical necessity documentation before starting treatment.
If you compete in any sport that drug-tests, this distinction matters. Using exogenous testosterone without an approved TUE is a violation, whether or not the use is medically necessary.
A TUE for documented hypogonadism is possible, but requires formal documentation of diagnosis and medical necessity. For competitive athletes reading this: get the diagnosis right first, then pursue the TUE pathway before starting treatment.
What Are the FDA-Approved Testosterone Treatments?
For reference — because this comes up in every conversation about symptoms. The FDA has approved multiple testosterone replacement products for male hypogonadism:
- Topical gels: Androgel (1% and 1.62%), Testim (1%)
- Injections: Depo-Testosterone (testosterone cypionate), Aveed (testosterone undecanoate)
- Nasal gel: Natesto
- Oral: Jatenzo (testosterone undecanoate capsules)
- Subcutaneous injection: Xyosted (testosterone enanthate)
These products are approved specifically for pathological hypogonadism (primary and hypogonadotropic) — not for age-related testosterone decline alone. Treatment decisions need to account for individual CVD risk, prostate health, fertility intentions, and hematocrit.
Frequently Asked Questions
What are the first signs of low testosterone in men?
The earliest symptoms are usually a noticeable drop in libido, persistent fatigue that doesn't improve with sleep, and decreased motivation or drive. Some men notice mood changes — irritability or a general flatness — before they notice sexual symptoms. These early signs tend to be gradual and get attributed to stress or age, which is part of why low testosterone is often diagnosed late.
What testosterone level is considered low?
The Endocrine Society defines low testosterone as below 300 ng/dL on two separate morning blood tests, in a man who also has symptoms of hypogonadism (Bhasin et al., 2010). A single measurement isn't sufficient for diagnosis. Some men feel symptoms at levels somewhat above this threshold, particularly if their free testosterone is also low due to high SHBG.
Can low testosterone cause depression?
Yes — and the association is stronger than most people realize. In the TRAVERSE trial, 50.8% of 5,204 hypogonadal men had significant depressive symptoms at baseline (Bhasin et al., 2024). Testosterone acts on mood-regulating brain circuits. TRT has shown modest but statistically significant mood improvements versus placebo in men with hypogonadism. But clinical depression needs full evaluation — testosterone is part of the picture, not the whole picture.
Can low testosterone cause sleep problems?
Low testosterone is associated with sleep disturbances, including reduced sleep quality and, in some cases, worsening of sleep apnea. The relationship also runs the other way: poor sleep, particularly obstructive sleep apnea, significantly suppresses testosterone. If you have poor sleep and low T, you may need to address both — starting TRT without treating untreated sleep apnea can worsen hematocrit and miss a reversible cause of the low testosterone itself.
At what age does testosterone start to decline?
Testosterone declines at approximately 1–2% per year after age 40 (Wu et al., 2010). By the 60s, roughly 20% of men have low total testosterone and about 30% have low free testosterone (Cunningham, 2006). The decline is gradual — which is exactly why men often don't recognize when it's crossed into clinically significant territory. Age alone doesn't cause hypogonadism in most men, but it does push susceptible men below the threshold.
What to Do If You Think You Have Low Testosterone Symptoms
The first step when low testosterone symptoms are suspected is not TRT — it is proper testing. That means two morning testosterone measurements (7–10 AM, on separate days), plus LH, FSH, free testosterone, and SHBG. Diagnosis requires both confirmed low levels below 300 ng/dL and the presence of symptoms (Bhasin et al., 2010). If both criteria are met, a clinical conversation about treatment options can begin.
If you've read through those symptom clusters and some of them sound familiar — fatigue, lower libido, muscle loss, flat mood — the next step isn't to assume you need TRT. It's to get your levels properly tested.
That means a morning blood draw (two, ideally, on separate days), full panel that includes total and free testosterone, LH, FSH, and likely SHBG. If your levels come back below 300 ng/dL and you have symptoms, that's when a real clinical conversation about options begins.
At HEXIS, we don't prescribe based on symptoms alone or a single borderline lab result. We look at your full hormone panel, your cardiovascular history, and your goals — because the right protocol for a 42-year-old with primary hypogonadism looks different from the right protocol for a 60-year-old with obesity-driven functional hypogonadism. In our clinical experience, the men who feel the most frustrated are those who've had one normal-range result at 2 PM and were told their "levels are fine" — often the most important follow-up question is simply: when was the blood drawn?
If you want a real evaluation from a licensed provider who will look at your actual numbers, schedule a consultation.
- 1
Low testosterone is defined as below 300 ng/dL on two morning measurements — with symptoms. You need both.
- 2
The five symptom clusters are sexual (libido, ED), energy/vitality, body composition, mood, and physical signs. Each has different evidence strength.
- 3
The TRAVERSE trial (n=5,204) is the largest RCT on TRT and confirms that testosterone therapy improves sexual function and mood versus placebo — with modest effect sizes.
- 4
50.8% of hypogonadal men in TRAVERSE had significant depressive symptoms — a pattern that often goes unrecognized.
- 5
For men with functional hypogonadism driven by obesity or sleep apnea, treating the underlying cause may normalize levels without TRT.
- 6
Diagnosis requires a full hormone panel, two morning draws, and a provider who will look at your actual numbers — not just a borderline result.