TRT Clinic Near You (Great Falls + Telehealth MT/WA/ID/OR)
TRT Clinic Near Me: Great Falls + Telehealth (MT/WA/ID/OR)
Not every TRT clinic is running the same playbook. Some follow established clinical guidelines — two morning blood draws, a full baseline panel, licensed prescriber, ongoing monitoring. Others skip most of that and hand you a prescription after a five-minute form. Knowing the difference protects your health and your money.
The short answer: A legitimate TRT clinic — whether in-person in Great Falls, MT or via telehealth across Montana, Washington, Idaho, or Oregon — diagnoses low testosterone using two separate morning blood draws with documented symptoms, checks your baseline PSA and hematocrit, and monitors your labs every 3–6 months. HEXIS Health does all of that. Here's exactly what to look for, and what to walk away from.
What Legitimate TRT Diagnosis Actually Looks Like
Two morning blood draws, documented symptoms, and a licensed prescriber who reviews both — that is the minimum standard for a legitimate TRT diagnosis, per the Endocrine Society's 2018 Clinical Practice Guideline (Bhasin et al., 2018).
Most men who call around asking about TRT have the same fear: they've been told their labs are "normal" and they still feel like garbage. The flip side is equally real — some clinics will hand you a prescription without doing the diagnostics that make testosterone therapy safe. Both problems have the same root: the diagnosis wasn't done right.
Testosterone has natural diurnal variation — it peaks in the morning and drops as the day goes on. That means a single afternoon draw can make your levels look lower than they actually are, which leads to prescriptions that aren't warranted. The guideline requires two separate measurements, both drawn in the morning, before any diagnosis is made (Bhasin et al., 2018).
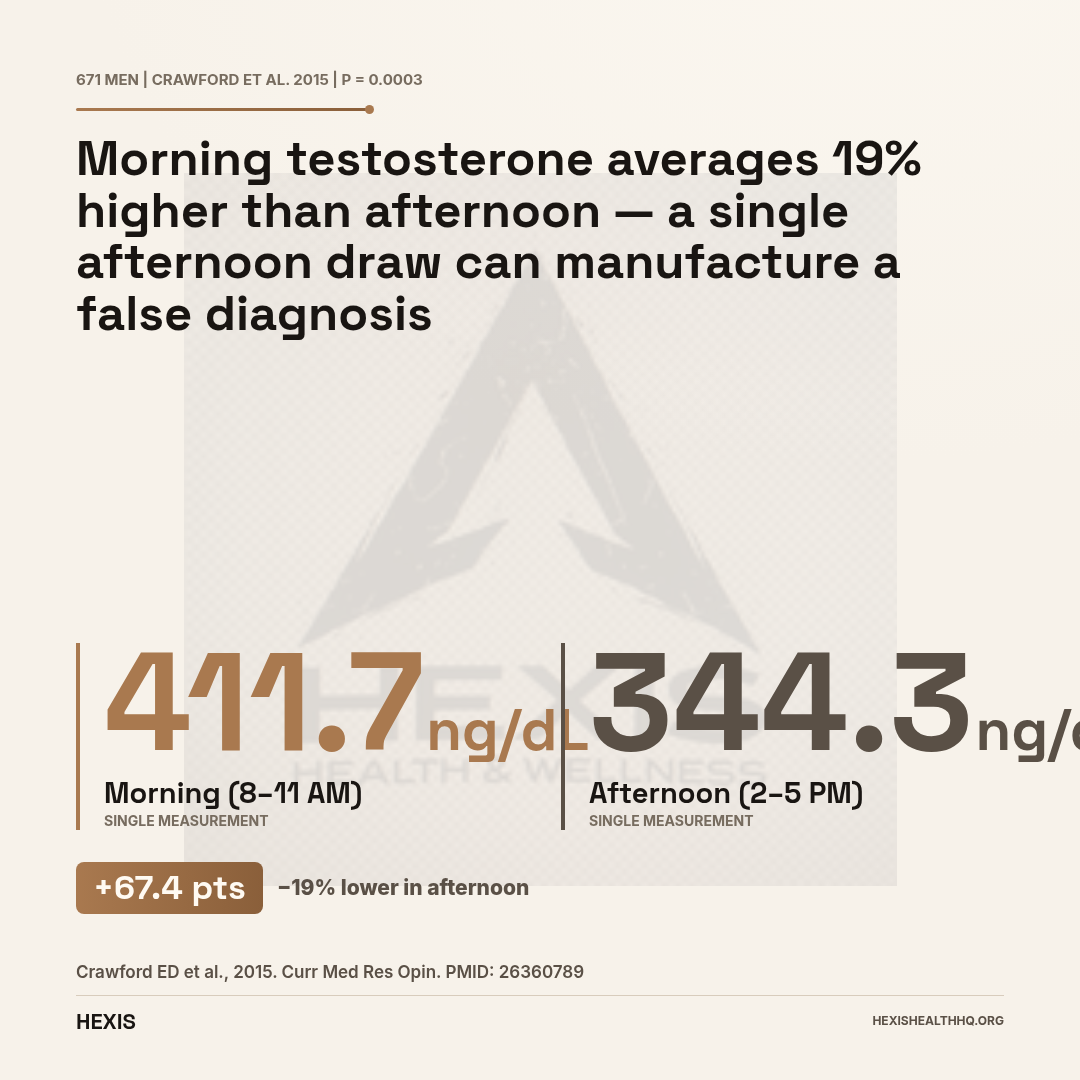
The data behind the morning-draw rule is concrete. In a study of 671 men, morning testosterone averaged 411.7 ng/dL versus 344.3 ng/dL in afternoon draws — a 19% difference, with p = 0.0003 (Crawford et al., 2015). A late-afternoon draw that comes back at 280 ng/dL might actually be 370 ng/dL if drawn correctly. Clinics that skip this step are flying blind.
The diagnostic threshold question gets murkier. The Endocrine Society recommends using each lab's own reference range rather than a fixed cutoff (Bhasin et al., 2018). The TRAVERSE trial — the largest TRT safety study ever conducted, with 5,204 men — used two draws below 300 ng/dL as its enrollment criterion (Bhasin et al., 2023). A 2017 harmonized reference analysis put the 2.5th percentile for healthy men at approximately 264 ng/dL, though that figure requires full-text verification for the exact number (Travison et al., 2017). The practical takeaway: low testosterone is not a single cutoff. It's a threshold that varies by lab method AND it only counts if you also have symptoms.
That last part matters. A lab number without symptoms isn't a diagnosis. Decreased libido, persistent fatigue, loss of muscle mass, depression, and erectile dysfunction are the clinical hallmarks of hypogonadism — and a legitimate clinic documents them before prescribing. Labs alone are not enough (Bhasin et al., 2018).
What Labs Should a TRT Clinic Order Before Prescribing?
A proper pre-TRT workup is not just a testosterone level — it is a full baseline panel covering PSA, hematocrit, CBC, metabolic panel, and estradiol, in addition to two morning testosterone draws.
Before any responsible provider writes a prescription, you should have total testosterone (two morning draws), PSA for men over 40, hematocrit, a complete blood count, metabolic panel, and estradiol:
PSA — The TRAVERSE trial excluded men with PSA above 3.0 ng/mL before enrollment, because elevated PSA can indicate prostate pathology that should be evaluated before starting TRT (Bhasin et al., 2023). Getting a baseline also gives your provider a reference point so that any future PSA rise can be assessed in context.
Hematocrit — Testosterone stimulates red blood cell production, which raises hematocrit. If hematocrit climbs too high, blood thickens and cardiovascular risk increases. The Canadian transfusion guideline recommends stopping TRT if hematocrit exceeds 54% (Chin-Yee et al., 2017). The European Academy of Andrology (EAA) considers hematocrit above 48–50% a relative contraindication to starting TRT at all (Corona et al., 2020). A clinic that never checks hematocrit isn't managing this risk — it's ignoring it.
Estradiol — Testosterone converts to estradiol in fat tissue, and some men experience gynecomastia, mood changes, or sexual dysfunction as estradiol rises during TRT. There's no established consensus cutoff for stopping TRT based on estradiol alone, so clinical judgment and symptom tracking are required here. Your provider should monitor and individualize.
If a clinic offers to start you on testosterone after a single lab value and a short online questionnaire, that's not a protocol — that's a liability.
In-Person vs Telehealth TRT
Is In-Person TRT Better Than Telehealth?
Neither in-person nor telehealth TRT is inherently better — both formats can meet the same diagnostic and monitoring standards. The critical variable is not the delivery method but whether the clinic orders the right labs, employs a licensed prescriber, and schedules follow-up monitoring.
Telehealth TRT has real advantages, especially for patients in rural and frontier areas like much of Montana, where driving two hours for a 20-minute appointment is a genuine barrier to care. Research shows that telehealth TRT can improve access to guideline-concordant treatment in underserved communities (Dubin et al., 2022). COVID-19 exposed this access problem sharply — barriers to receiving TRT in community settings increased significantly during the pandemic, pushing more patients toward remote options (Troesch et al., 2021). For follow-up visits once your protocol is established and your labs are stable, telehealth is often the right tool.
The regulatory side has some nuance worth knowing. Testosterone is a Schedule III controlled substance. The Ryan Haight Online Pharmacy Consumer Protection Act historically required an in-person evaluation before a controlled substance could be prescribed via telemedicine. The DEA issued a COVID-era waiver that relaxed that requirement from 2020 through 2023. That waiver has ended, and the DEA is now finalizing a special telemedicine registration framework that legitimate platforms must comply with (Kannarkat et al., 2023). A provider prescribing testosterone via telehealth today needs to either have met you in person at some point or hold specific DEA telemedicine authorization. No workaround exists for that requirement.
There's a harder issue with direct-to-consumer (DTC) testosterone platforms specifically. A study evaluating men who sought care through DTC internet prescription platforms found that these services missed significant underlying pathology in approximately 40% of cases — conditions that would have been caught during a traditional office evaluation (Shahinyan et al., 2020). The most common problem: DTC platforms focus on symptom questionnaires and testosterone levels while skipping the physical and laboratory findings that reveal secondary hypogonadism, testicular pathology, or other treatable root causes.
Telehealth TRT from a legitimate clinic is not the same thing as a DTC platform. The difference is whether a licensed prescriber reviews your full baseline panel, conducts a video consultation where they're actually looking at you, and follows up with monitoring labs. For HEXIS patients outside Great Falls — across Montana, Washington, Idaho, or Oregon — telehealth appointments include all of that.
You can read more about the specific online TRT process in our article on online TRT options.
Red Flags That Signal a T Mill
A "T mill" is a testosterone clinic — in-person or online — that prescribes based on convenience rather than clinical standards: no two-draw diagnosis, no baseline monitoring, and no licensed prescriber reviewing your actual results. Ten specific red flags distinguish these operations from legitimate providers.
Walk away if a clinic does any of the following:
- Prescribes testosterone without two separate morning draws on different days
- Does not document clinical symptoms before prescribing — treats a single lab value as sufficient
- Does not check baseline PSA in men over 40
- Does not test hematocrit before starting or during treatment
- Guarantees a prescription before reviewing your labs
- Has no licensed MD, DO, NP, or PA who personally reviews your results
- Uses telehealth without any in-person contact or valid DEA telemedicine authorization
- Does not discuss cardiovascular risk, fertility implications, or TRAVERSE safety data
- Does not schedule follow-up monitoring labs
- Does not perform a digital rectal exam (DRE) or refer for prostate evaluation when PSA or symptoms warrant it
These aren't nitpicky technicalities. Each one represents a point where a clinic is choosing convenience over safety. Missing a baseline PSA can leave prostate cancer undetected. Skipping hematocrit monitoring can lead to polycythemia that goes unaddressed. A clinic that doesn't document symptoms is essentially admitting it hasn't ruled out secondary causes of low T — thyroid dysfunction, sleep apnea, pituitary adenoma — that might resolve without testosterone at all.
For a full breakdown of how low testosterone is evaluated and treated, see our guide on how to treat low testosterone.
Testosterone raises red blood cell production. If hematocrit climbs above 48–50%, it's a relative contraindication to starting TRT. If it exceeds 54% during treatment, therapy should be paused or the dose reduced — thickened blood raises cardiovascular risk.
Source: EAA Guidelines (Corona et al., 2020, PMID 32026626); Canadian guideline (Chin-Yee et al., 2017, PMID 28150363)
How Often Should You Get Labs Checked on TRT?
Follow-up labs at 3–6 months after starting TRT, then annually once your protocol is stable — that is the Endocrine Society's monitoring schedule, and every check should include hematocrit, PSA, and testosterone level (Bhasin et al., 2018).
Starting TRT is not a set-it-and-forget-it event. Your body's response to testosterone is individual — some men see hematocrit rise quickly, others barely move; some need estradiol management, others never do. Monitoring is how your provider catches those changes before they become problems.
That monitoring schedule should include testosterone level, hematocrit, and PSA at minimum. If symptoms suggest estradiol issues — gynecomastia, water retention, emotional lability — estradiol gets added to the panel.
If hematocrit exceeds 54%, TRT should be paused or the dose reduced while the elevation resolves (Chin-Yee et al., 2017). This is not a rare event — polycythemia is one of the most common adverse effects of testosterone therapy, and it's entirely manageable if monitored. It becomes dangerous when it goes undetected because nobody was checking.
For men of reproductive age, there's another conversation that should happen at the start: testosterone therapy suppresses the body's natural gonadotropin production, which reduces sperm production and can cause infertility. That doesn't mean TRT and fertility are incompatible — but it means a legitimate clinic will have that conversation and discuss alternatives like clomiphene or HCG if fertility preservation matters to you.
Athletes should also know that testosterone is a prohibited substance under the World Anti-Doping Agency (WADA) S1 classification regardless of medical need. A Therapeutic Use Exemption (TUE) is available for documented hypogonadism, but that process requires clear documentation from a treating provider.
To understand the full range of what to expect from treatment — including timeline and side effect management — see our detailed guide on TRT side effects and what to expect.
HEXIS Health in Great Falls, MT: In-Person + Telehealth TRT
HEXIS Health provides in-person TRT care in Great Falls, Montana and telehealth TRT across Montana, Washington, Idaho, and Oregon. Every patient starts the same way: two fasting morning testosterone draws before a prescriber reviews anything — because that is the standard, and shortcuts in diagnosis create problems down the line.
If you're in Great Falls or anywhere in Cascade County, you can come in for the full in-person workup: testosterone, PSA, hematocrit, CBC, metabolic panel, and estradiol — all reviewed by a licensed prescriber before any protocol is built. There is no prescription before the labs, and there is no protocol without a conversation about your symptoms.
For patients who can't make it to Great Falls, telehealth appointments include a video consultation with your provider, not a questionnaire routed to an algorithm. Follow-up monitoring is built into every protocol. Your labs come back, your provider reviews them, and your protocol adjusts when the numbers warrant it.
The distinction from a DTC platform is real: we're a medical practice, not a subscription service. Your provider knows your file.
Schedule a consultation at HEXIS Health to get your baseline labs and talk through what testosterone therapy would actually look like for you.
Frequently Asked Questions
What blood tests should a TRT clinic order before prescribing?
Before prescribing testosterone, a legitimate clinic should order at minimum: total testosterone (two separate morning draws), PSA (for men over 40), hematocrit, complete blood count, metabolic panel, and estradiol. The Endocrine Society guideline requires both low lab values AND documented symptoms before a diagnosis is made (Bhasin et al., 2018). A single testosterone draw or a questionnaire alone is not sufficient for diagnosis.
Do I really need two blood draws before starting TRT?
Yes. Testosterone levels vary significantly across the day — averaging 411.7 ng/dL in morning draws versus 344.3 ng/dL in afternoon draws in one 671-patient study (Crawford et al., 2015). A single low result may reflect timing rather than true deficiency. Both the Endocrine Society (Bhasin et al., 2018) and the European Academy of Andrology (Corona et al., 2020) require two separate morning measurements before a diagnosis of hypogonadism is confirmed.
Is telehealth TRT legitimate and safe?
Telehealth TRT from a licensed medical practice — where a real provider reviews your full panel, conducts a video consultation, and schedules monitoring labs — is a legitimate care model that improves access for rural and frontier patients (Dubin et al., 2022). The risk comes from DTC platforms that skip the evaluation. Research found these services missed significant pathology in roughly 40% of men evaluated (Shahinyan et al., 2020). The format is not the problem; the standards are.
What are the red flags of a bad TRT clinic?
The clearest red flags: prescribing without two morning draws, no baseline PSA for men over 40, no hematocrit monitoring, no documentation of symptoms, guaranteeing a prescription before lab review, and no licensed prescriber personally reviewing your results. A clinic that doesn't build in follow-up monitoring labs — every 3–6 months for the first year — is not managing the known risks of TRT (Chin-Yee et al., 2017).
Does HEXIS offer telehealth TRT in Montana, Washington, Idaho, or Oregon?
Yes. HEXIS Health provides telehealth TRT services across Montana, Washington, Idaho, and Oregon, in addition to in-person care in Great Falls, MT. Telehealth appointments include a video consultation with a licensed provider, full baseline lab review, and a structured monitoring schedule. Prescribers are licensed in each state they serve and operate within the current DEA telemedicine regulatory framework (Kannarkat et al., 2023).
This article is for informational purposes and does not constitute medical advice. Testosterone replacement therapy is a prescription treatment that requires evaluation by a licensed medical provider. If you have questions about your hormone levels or symptoms, consult a qualified healthcare professional.
- 1
Two fasting morning testosterone draws — both below threshold — before any prescription
- 2
Documented symptoms alongside low labs (libido, fatigue, muscle loss, ED, depression)
- 3
Baseline PSA (men 40+), hematocrit, CBC, metabolic panel, and estradiol
- 4
Licensed prescriber who reviews results personally — not an algorithm
- 5
Follow-up labs at 3–6 months, then annually; hematocrit stop at 54%
- 6
Telehealth providers: DEA-authorized and licensed in your state