What Causes Low Testosterone in Men? Primary, Secondary, and Functional Hypogonadism Explained
What Causes Low Testosterone in Men?
Your doctor told you your testosterone is low. But low compared to what, and — more importantly — why is it low? Those two questions are not the same thing, and the answer to the second one determines what actually gets done about it.
There are over a dozen distinct reasons testosterone can drop, and they fall into three fundamentally different categories. Figuring out which one applies to you is the entire point of the diagnostic workup.
The short answer: Low testosterone has three main root causes — testicular failure (primary hypogonadism), a signaling problem in the brain or pituitary gland (secondary hypogonadism), and reversible lifestyle-driven suppression (functional hypogonadism). A single blood test measuring LH and FSH alongside testosterone tells your provider which category you fall into and, critically, whether the cause is structural or reversible. Without those two extra numbers, any diagnosis is incomplete (Bhasin et al., 2018).
What Your LH and FSH Results Tell You
The lab pattern that localizes where the problem is
| Pattern | Interpretation | Next Step | |
|---|---|---|---|
| Low T + HIGH LH + HIGH FSH | Primary hypogonadism | Testes are failing — pituitary signal is normal | Rule out Klinefelter, chemo damage, orchitis |
| Low T + LOW/NORMAL LH + LOW/NORMAL FSH | Secondary hypogonadism | Signal is failing — testes could work if told to | Check prolactin, consider pituitary imaging |
| Low T + Low LH + metabolic risk | Functional hypogonadism | Reversible suppression — no structural lesion | Address obesity, opioids, sleep apnea first |
Source: Bhasin et al., 2018. Endocrine Society Clinical Practice Guideline. PMID 29562364.
The Diagnostic Framework: Why LH and FSH Are the Key
Most people get one number back from their doctor: total testosterone. That number tells you that something is wrong. It does not tell you why.
Luteinizing hormone (LH) and follicle-stimulating hormone (FSH) are the messengers your pituitary gland sends to your testes, signaling them to produce testosterone. When you add those two values to your testosterone result, the pattern tells a completely different story depending on which piece of the system has failed.
High LH + High FSH + Low T = Primary hypogonadism. The pituitary is shouting the signal at full volume. The testes aren't responding. The problem is in the testes themselves — damaged, undeveloped, or genetically compromised.
Low or normal LH + Low or normal FSH + Low T = Secondary hypogonadism. The pituitary isn't sending the signal at all, or it's sending it too weakly. The testes could probably work fine if they received the message — but they're not getting it. The problem is upstream, in the hypothalamus or pituitary.
This framework is the backbone of the Endocrine Society's clinical practice guidelines on hypogonadism (Bhasin et al., 2018). Without it, providers are guessing.
Primary Hypogonadism: When the Testes Are the Problem
Primary hypogonadism — also called hypergonadotropic hypogonadism — means the testes have failed. The pituitary is doing its job perfectly; the signal is reaching the testes, but testosterone production still falls short. Because the pituitary keeps trying to compensate, LH and FSH go high.
Klinefelter Syndrome: The Most Common Genetic Cause
Klinefelter syndrome (47,XXY karyotype) affects approximately 1 in 500–600 males, making it the most frequent chromosomal cause of primary hypogonadism (Gravholt et al., 2018). Most men with Klinefelter syndrome are never formally diagnosed.
The extra X chromosome doesn't prevent the testes from forming — but it disrupts the seminiferous tubules and Leydig cell function, progressively impairing testosterone production after puberty. About 50% of men with Klinefelter syndrome have testosterone within the normal range without treatment; the other half require testosterone replacement (Gravholt et al., 2018).
Physically, the signs include small, firm testes, often some breast tissue development (gynecomastia), and near-universal infertility from severely impaired sperm production.
Chemotherapy and Radiation
Alkylating chemotherapy agents and testicular radiation cause direct Leydig cell toxicity. The degree of damage depends on the agent, dose, and whether radiation was directed at the testes. In many cases the damage is permanent — the testes cannot recover their previous testosterone output even years after treatment ends.
Men who received cancer treatment in childhood or young adulthood should have testosterone checked periodically, since the functional impact can evolve over decades (Bhasin et al., 2018).
Mumps Orchitis, Testicular Injury, and Torsion
Viral orchitis — most commonly from mumps — causes testicular inflammation that can destroy Leydig cells. About 30% of post-pubertal men who develop mumps orchitis will have some degree of testicular atrophy; a meaningful proportion develop hypogonadism.
Testicular torsion, physical trauma, and autoimmune orchitis are less common causes that follow the same pattern: direct damage to the testosterone-producing tissue inside the testes.
These causes share the same lab signature — low T, elevated LH and FSH — because the pituitary is intact and responding normally to the testicular failure.
Secondary Hypogonadism: When the Signal Fails
In secondary hypogonadism, the testes can make testosterone — they're just not getting the signal to do it. LH and FSH are low or inappropriately normal. The fault is upstream: the hypothalamus isn't pulsing GnRH properly, or the pituitary isn't releasing enough LH and FSH in response. This category includes both structural causes (pituitary tumors, Kallmann syndrome) and drug-induced suppression (opioids, glucocorticoids).
Pituitary Tumors and Hyperprolactinemia
Pituitary adenomas — benign tumors of the pituitary gland — are the most common structural cause of secondary hypogonadism. A large non-functioning adenoma physically compresses the gonadotroph cells that produce LH and FSH, reducing their output.
Prolactinomas are a specific type of functional pituitary tumor that produce excess prolactin. Elevated prolactin suppresses GnRH pulsatility at the hypothalamic level, which lowers LH and FSH, which drops testosterone. Prolactinomas are the most common functional pituitary tumor in men, and they account for a significant share of secondary hypogonadism cases (Bhasin et al., 2018).
Hyperprolactinemia is treatable. Dopamine agonists like cabergoline normalize prolactin levels, which allows the GnRH → LH → testosterone chain to recover. Checking prolactin is standard in any secondary hypogonadism workup — and this is one reason why.
Kallmann Syndrome and Congenital Hypogonadotropic Hypogonadism
Kallmann syndrome is a rare congenital condition affecting roughly 1 in 10,000–30,000 males, caused by the failure of GnRH-secreting neurons to migrate properly during fetal development. The defining feature beyond absent puberty is anosmia — the complete absence of the sense of smell — because the olfactory neurons and GnRH neurons share the same developmental migration pathway.
Kallmann syndrome is the most recognized subtype of congenital hypogonadotropic hypogonadism (CHH). A 2025 systematic review identified 93 genes associated with CHH presentations in males, of which 29 were unequivocally disease-causing (Castro et al., 2025). The condition is treatable — gonadotropin therapy or pulsatile GnRH can induce puberty and, in some cases, fertility. Spontaneous reversal occurs in a small minority of cases (roughly 10–20%).
Men with Kallmann syndrome present at puberty with failure to develop secondary sexual characteristics, very low LH and FSH, and very low testosterone.
Head Trauma and Infiltrative Disease
Traumatic brain injury — even concussions that seemed minor at the time — can disrupt pituitary function. Hypopituitarism following TBI is underdiagnosed, partly because the hormonal effects may not become apparent for months or years.
Hemochromatosis (iron overload) causes iron deposition in pituitary gonadotroph cells, directly impairing LH and FSH secretion. A significant share of untreated cases develop hypogonadism as a result. Phlebotomy reduces iron load but pituitary recovery is variable.
Chronic opioid use suppresses GnRH at the hypothalamus — producing secondary hypogonadism with low LH, low FSH, and low testosterone. Men on long-term opioids for pain are rarely screened for this effect, despite multiple studies reporting significant rates of testosterone suppression. The pattern is reversible in most cases when opioids are stopped or reduced.
Source: De Maddalena et al., 2012. Pain Physician. PMID 22786450.
Functional Hypogonadism: Reversible Suppression With No Structural Lesion
Functional hypogonadism is the most potentially reversible form of low testosterone — and the most commonly missed. The HPG axis isn't structurally damaged. It's being suppressed by something systemic: excess body fat, chronic opioids, untreated sleep apnea, metabolic disease. Remove the suppression, and testosterone can recover without TRT.
Among men under 60, this is increasingly recognized as the most prevalent form of low testosterone — and the one most often labeled "unexplained" when the real cause is sitting right there in the medication list or the metabolic panel (Corona et al., 2020).
Obesity and the Aromatase Mechanism
Fat tissue is metabolically active. Adipose cells express aromatase, the enzyme that converts testosterone into estradiol. The more fat tissue you carry, the more testosterone gets converted before it can circulate and do its job.
Elevated estradiol then feeds back to the hypothalamus and pituitary, suppressing GnRH and LH release. This drops LH further, which means even less testosterone gets signaled. It's a self-reinforcing cycle: excess fat lowers testosterone, and lower testosterone promotes fat accumulation by reducing lean mass and metabolic rate (Mohr et al., 2006).
Both directions of that cycle have solid evidence behind them. The European Academy of Andrology is direct about it: for men with functional hypogonadism driven by obesity, weight loss comes first — TRT should not be the opening move (Corona et al., 2020).
Men with obesity and low testosterone often have low LH as well — the secondary pattern — because aromatase-driven estrogen is suppressing the signal.
Opioid-Induced Hypogonadism
Opioids suppress GnRH pulsatility at the hypothalamic level, producing a clean secondary hypogonadism pattern: low LH, low FSH, low testosterone. This is not a minor or rare effect — multiple studies report significant rates of testosterone suppression among men on chronic opioid therapy (De Maddalena et al., 2012; Vuong et al., 2010).
The effect appears dose-dependent and occurs with both oral and intrathecal opioids. Men on opioids for chronic pain who develop fatigue, loss of libido, depression, or difficulty building or maintaining muscle should have their hormone panel checked.
Opioid-induced hypogonadism is generally reversible if the opioids are discontinued or the dose substantially reduced. Recovery typically occurs within weeks to months of cessation (De Maddalena et al., 2012).
This is one of the most clinically important causes to identify because it has a clear, addressable root cause and because men on opioids are rarely screened for hormonal effects.
Type 2 Diabetes and Insulin Resistance
Low testosterone and type 2 diabetes travel together. The relationship is bidirectional: insulin resistance impairs Leydig cell steroidogenesis, and low testosterone worsens insulin sensitivity.
Population studies consistently show higher rates of hypogonadism among men with type 2 diabetes compared to age-matched controls. Metabolic syndrome — the cluster of abdominal obesity, elevated triglycerides, low HDL, hypertension, and impaired fasting glucose — compounds the risk through multiple overlapping mechanisms (Harman et al., 2001).
Improving glycemic control and metabolic health can partially restore testosterone. That doesn't always bring T fully back into range, but it's a relevant first move for any man carrying both diagnoses.
Obstructive Sleep Apnea
Testosterone is largely produced during sleep, particularly during REM sleep. Chronic obstructive sleep apnea disrupts normal nocturnal LH pulsatility by causing repeated hypoxic episodes throughout the night. The result is impaired overnight testosterone synthesis.
Men with untreated OSA consistently show lower testosterone compared to matched controls. CPAP therapy — treating the sleep apnea — can partially restore testosterone in some men, though the magnitude of improvement is modest and not universal. Still, it's worth diagnosing and treating OSA before starting testosterone replacement, since the sleep disorder is the underlying driver.
Chronic Stress and Glucocorticoids
Both exogenous glucocorticoids (prescribed corticosteroids like prednisone) and endogenous cortisol suppress the HPG axis at multiple levels. Cortisol inhibits GnRH pulsatility at the hypothalamus and LH secretion at the pituitary, and directly impairs Leydig cell testosterone synthesis.
Men on long-term steroid therapy — for asthma, autoimmune conditions, or inflammatory diseases — should be monitored for hypogonadism. The effect is dose-dependent. Like opioid-induced hypogonadism, it generally reverses when the steroid is discontinued or the dose reduced, though complete recovery isn't guaranteed.
Chronic psychological stress raises cortisol chronically enough to have measurable effects on testosterone through the same mechanism.
Alcohol and Testosterone
Heavy, chronic alcohol use impairs testosterone through multiple pathways: direct Leydig cell toxicity, increased aromatase activity (more T converted to estrogen), and suppression of GnRH secretion. Men with alcohol use disorder consistently show lower testosterone than matched non-drinkers.
Unlike some functional causes, the effect of chronic alcohol is not always fully reversible — prolonged heavy use can cause direct Leydig cell damage that resembles primary hypogonadism even though the initiating mechanism was central.
Age-Related Testosterone Decline: A Category of Its Own
Testosterone declines gradually with age — roughly 1–2% per year after age 30 to 40 in population studies, based on data from the Massachusetts Male Aging Study and the Baltimore Longitudinal Study of Aging (Harman et al., 2001). This is not a disease. It is a normal biological process.
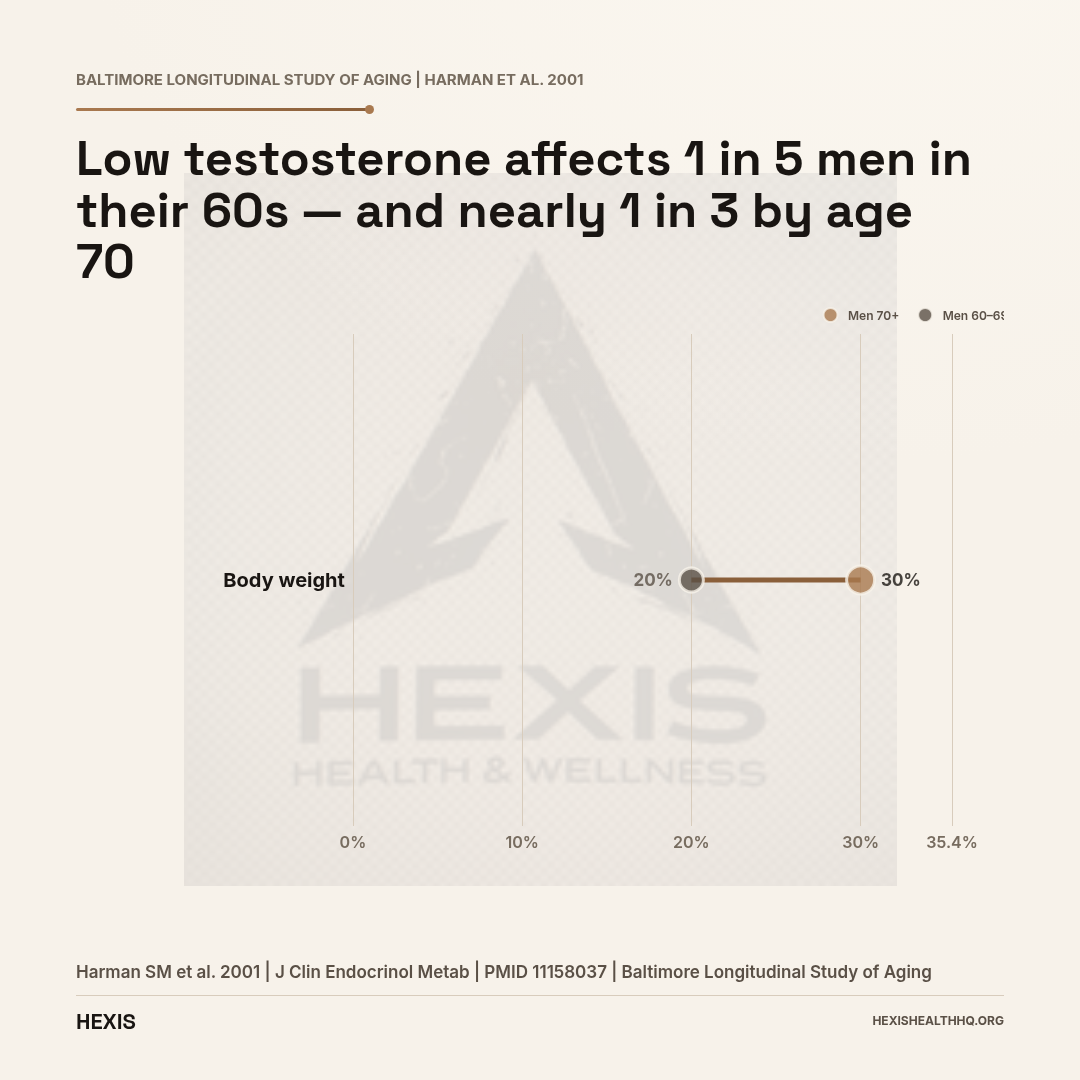
About 20% of men aged 60–69 have testosterone below the clinical threshold for hypogonadism, and about 30% of men 70 and older fall in that range (Harman et al., 2001).
Age-related decline has two overlapping components. There's a primary component — Leydig cell mass and function decrease over time, reducing the testes' testosterone output. And there's a secondary component — GnRH pulsatility from the hypothalamus becomes less consistent with age, reducing the signal to the pituitary. Because both components contribute, LH may be mildly elevated or normal in older men with low T (Yeap et al., 2024).
The clinical concept of late-onset hypogonadism (LOH) refers specifically to symptomatic men who are older, biochemically low in testosterone, and have no other identifiable cause. It is a diagnosis of exclusion — meaning every other category on this page needs to be ruled out first.
That last part matters. Age alone is a risk factor, not a complete explanation. A 65-year-old with low T and undiagnosed sleep apnea, or who's been on opioids for back pain, doesn't have late-onset hypogonadism — he has a functional cause that might be addressable.
What Medications Can Lower Your Testosterone?
Six drug classes are known to suppress testosterone, and they account for a meaningful share of low-T diagnoses that could be addressed by changing a prescription rather than starting TRT:
Opioids — the most clinically significant, discussed above.
Exogenous androgens and anabolic steroids — taking testosterone from outside sources completely shuts down the HPG axis. The pituitary detects high androgens, stops secreting LH, and the testes go quiet. Men who stop using anabolic steroids often experience a prolonged recovery period because the axis suppression can persist for months.
Glucocorticoids — prednisone, dexamethasone, and similar agents suppress the axis at multiple levels (discussed above).
Ketoconazole — an antifungal that blocks steroidogenesis enzymes. Used at high doses, it significantly reduces testosterone production.
Certain antipsychotics and antidepressants — particularly medications that elevate prolactin as a side effect. High prolactin suppresses GnRH, producing secondary hypogonadism. Risperidone, haloperidol, and some other antipsychotics are known prolactin-elevating agents.
GnRH agonists — intentionally used to suppress testosterone in prostate cancer treatment. Not a side effect — this is the mechanism of action.
If you're taking any of these medications and have low testosterone, medication review is an essential part of the workup before attributing the cause elsewhere.
How Is Low Testosterone Diagnosed? The Full Workup
The correct workup for low testosterone requires at minimum four lab values: total testosterone (on two separate morning fasting draws), LH, FSH, and prolactin. The Endocrine Society mandates two draws because testosterone varies significantly by time of day and between tests — and LH, FSH, and prolactin together localize whether the failure is at the testes, the pituitary, or a reversible systemic cause (Bhasin et al., 2018).
What that panel tells you:
- Total T low + LH high + FSH high → primary hypogonadism (testicular failure) → next step is karyotype if cause unclear, rule out Klinefelter
- Total T low + LH low/normal + FSH low/normal → secondary or functional hypogonadism → add prolactin, MRI pituitary if prolactin elevated or secondary cause unexplained
- Total T low + age + metabolic risk factors + low LH → functional hypogonadism → address root causes before considering TRT
This matters practically. A man with a pituitary adenoma compressing his gonadotrophs doesn't need TRT — he needs pituitary imaging and possibly surgery or medication to address the mass. A man with opioid-induced hypogonadism might recover completely without TRT once his pain regimen changes.
Treatment follows diagnosis, not the other way around. And the right diagnosis requires the right tests (Bhasin et al., 2010).
To understand what low testosterone actually feels like day-to-day, see our guide to low testosterone symptoms in men. If you're already past the "why is it low" question and want to understand treatment options, read how to treat low testosterone. For a detailed breakdown of what normal testosterone levels look like by decade, see testosterone levels by age.
Frequently Asked Questions
What is the difference between primary and secondary low testosterone?
Primary hypogonadism means the testes themselves are failing — the pituitary is sending signals normally (LH and FSH are high), but the testes aren't responding with adequate testosterone production. Secondary hypogonadism means the signal is the problem: the pituitary or hypothalamus isn't sending enough LH or FSH, so the testes never get the instruction to produce testosterone in the first place.
Can opioid pain medications cause low testosterone?
Yes. Opioids suppress GnRH pulsatility at the hypothalamic level, which reduces LH and FSH, which drops testosterone. This is a well-documented and underdiagnosed cause of low testosterone in men on chronic opioid therapy. Multiple reviews report significant rates of testosterone suppression with prolonged opioid use (De Maddalena et al., 2012; McGuirt et al., 2024). The effect is generally reversible when opioids are stopped.
Does obesity cause low testosterone, or does low testosterone cause obesity?
Both. Excess fat tissue contains aromatase, which converts testosterone into estradiol. More estradiol suppresses LH and GnRH, producing less testosterone. Meanwhile, lower testosterone promotes fat accumulation by reducing lean mass and slowing metabolism. It's a bidirectional cycle — each condition worsens the other (Mohr et al., 2006).
What blood tests tell you why testosterone is low?
Testosterone alone doesn't explain the cause. The full diagnostic panel includes total testosterone (two morning fasting draws), LH, FSH, and prolactin. High LH/FSH points to primary hypogonadism (testicular failure). Low or inappropriately normal LH/FSH points to secondary or functional hypogonadism (signaling failure). Elevated prolactin specifically points toward a pituitary adenoma or medication side effect (Bhasin et al., 2018).
Is age-related testosterone decline the same as hypogonadism?
Not exactly. Testosterone naturally declines about 1–2% per year after age 30 — that's aging biology, not a disease. Clinical hypogonadism in older men (late-onset hypogonadism) means having both biochemically low testosterone AND symptoms attributable to it, with no other identifiable cause. It's a diagnosis of exclusion. Many older men with low testosterone have an underlying cause — sleep apnea, opioids, obesity — that should be identified and addressed before attributing everything to age (Harman et al., 2001).
Work With a Provider Who Starts With the Right Tests
If you've been told your testosterone is low, the next question your provider should be asking is why. That answer lives in your LH, FSH, and prolactin — not just your total T. Understanding whether you have primary, secondary, or functional hypogonadism determines everything that comes after: whether lifestyle changes might solve it, whether a medication is suppressing your hormones, whether a pituitary scan is warranted, or whether testosterone replacement actually makes sense for your situation.
At HEXIS, we start with a full panel — not just a single testosterone number. Your LH, FSH, prolactin, and testosterone tell a story, and we want to read the whole thing before making any recommendations. Schedule a consultation if you want a provider who treats the cause, not just the number.
- 1
Primary hypogonadism (high LH+FSH): the testes have failed — Klinefelter, chemo, orchitis, torsion.
- 2
Secondary hypogonadism (low/normal LH+FSH): the signal has failed — pituitary tumor, prolactinoma, Kallmann, TBI.
- 3
Functional hypogonadism: reversible suppression — obesity, opioids, sleep apnea, glucocorticoids.
- 4
Age-related decline (LOH): gradual, both primary and secondary components — diagnosis of exclusion.
- 5
The workup requires total T + LH + FSH + prolactin. One number is not enough.