TRT Side Effects & Safety: What the Evidence Actually Shows
TRT Side Effects & Safety: What the Evidence Actually Shows
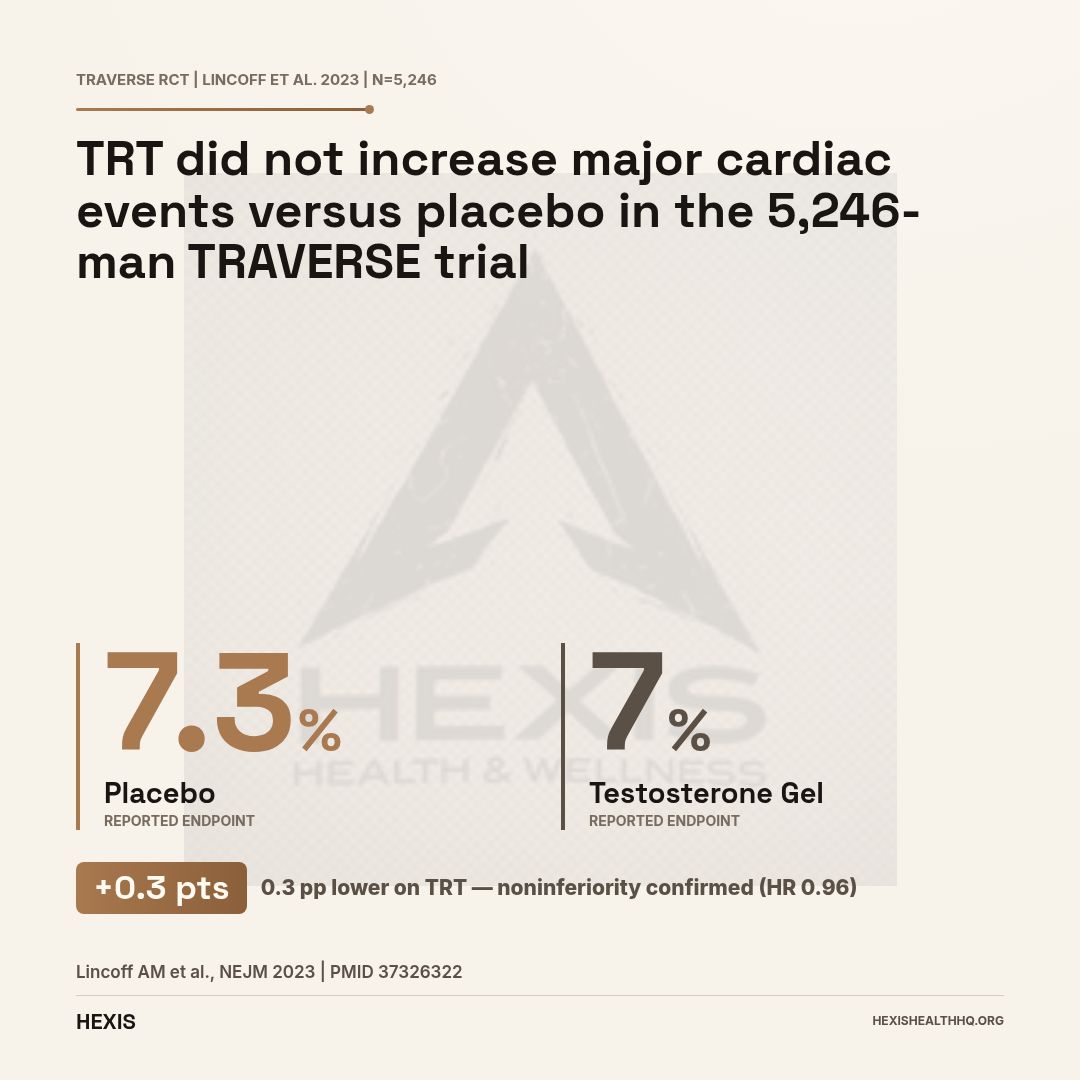
TRT's most common side effects are erythrocytosis (elevated red blood cell count), estradiol-driven gynecomastia, and HPG-axis suppression affecting fertility. Cardiovascular events were not increased in the 5,246-man TRAVERSE trial (Lincoff et al., 2023). Most effects are dose-dependent, formulation-dependent, and manageable with the monitoring protocol every TRT prescription should include.
TRT side effects get discussed at both extremes — dismissed as minor inconveniences or treated as reasons no one should ever touch the stuff. The evidence sits in between, and what follows breaks it down by effect type, starting with the question that comes up first in almost every conversation about TRT.
TRAVERSE (n=5,246): TRT vs placebo for major cardiac events — noninferiority confirmed. MACE 7.0% on TRT vs 7.3% on placebo (Lincoff et al., 2023)
Is TRT Safe for Your Heart?
For most men with diagnosed hypogonadism, the answer from the largest trial ever conducted is: yes, with one important nuance.
The TRAVERSE trial (NCT03518034) enrolled 5,246 men aged 45–80 with low testosterone and either existing cardiovascular disease or high cardiovascular risk. Half received testosterone gel; half received placebo. Primary cardiovascular events — heart attack, stroke, or cardiovascular death — occurred in 7.0% of the testosterone group versus 7.3% of the placebo group (HR 0.96; 95% CI, 0.78–1.17). That noninferiority finding was statistically significant (Lincoff et al., 2023). TRT did not increase major cardiac events even in men who already had cardiovascular disease.
But TRAVERSE also surfaced two signals that are worth sitting with.
Atrial fibrillation occurred in 3.5% of the testosterone group versus 2.4% on placebo. Pulmonary embolism occurred in 0.9% versus 0.5%. Neither was elevated enough to cancel the noninferiority finding, but both were elevated enough that the Androgen Society acknowledged them explicitly in their post-TRAVERSE position paper (Morgentaler et al., 2024).
A separate real-world analysis of 117,908 men with hypogonadism confirmed the cardiovascular picture — treated men had a lower risk of myocardial infarction (HR 0.94; 95% CI 0.89–0.99) but higher atrial fibrillation and VTE risk compared with propensity-matched untreated men (Bonnet et al., 2025).
TRT is not the cardiac time bomb the 2015 FDA label implied. But if you have a history of AFib or clotting disorders, your prescribing clinician needs to know that before you start.
Erythrocytosis: The Most Common Reason TRT Gets Stopped
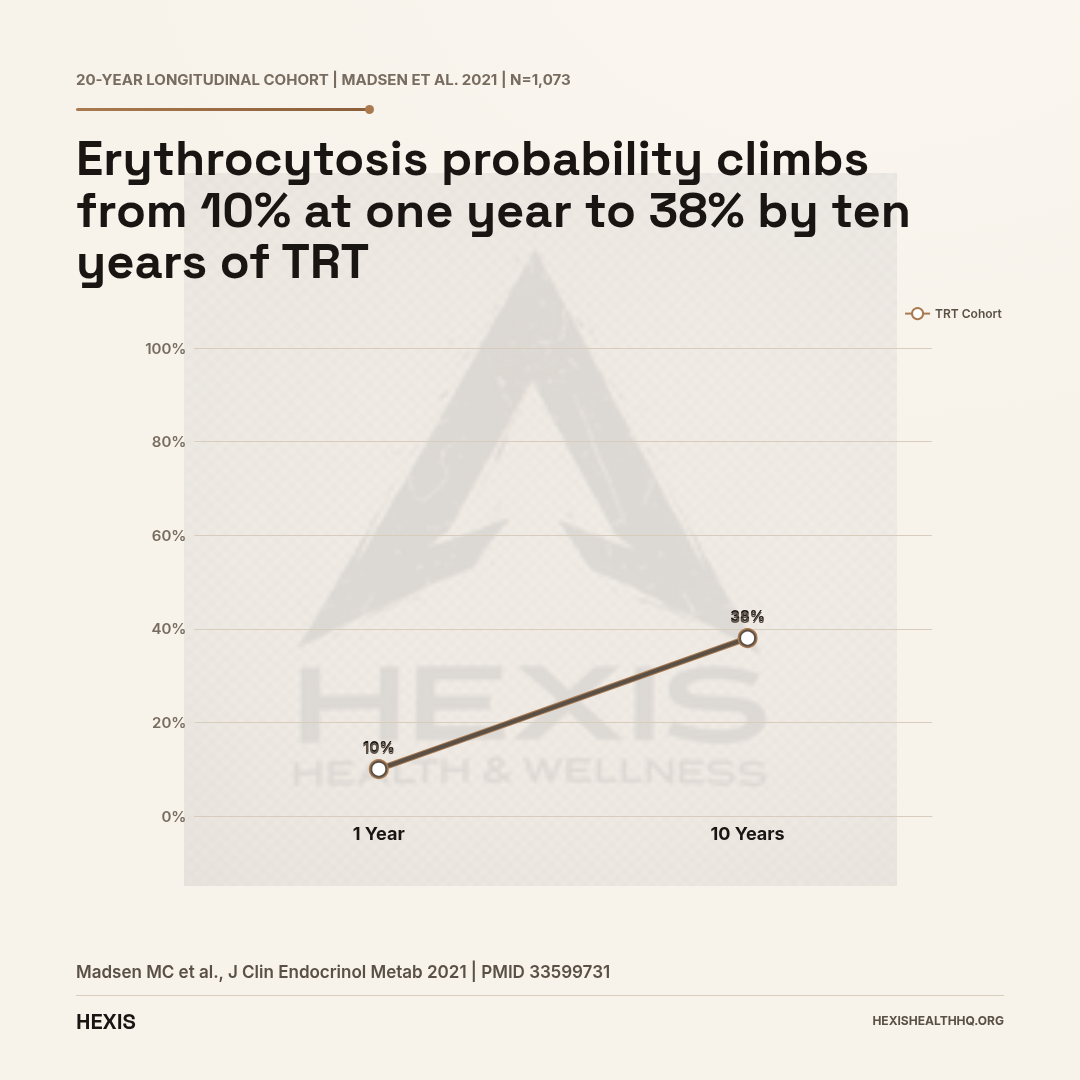
In a 20-year longitudinal study of 1,073 people on testosterone, erythrocytosis probability reached 10% at year one and 38% at year ten. Long-acting testosterone undecanoate carries 2.9× the risk of shorter-acting formulations. At hematocrit ≥54%, dose reduction or formulation switch is required.
Check hematocrit at baseline, 3–6 months, and annually. If it exceeds 54%, reduce dose, switch to a lower-peak formulation, or pause therapy.
Source: Defreyne et al., J Clin Endocrinol Metab, 2021 (PMID 33599731); Gianfrilli et al., Andrology, 2024 (PMID 39882268)
Erythrocytosis: The Most Common Reason People Stop TRT
Erythrocytosis — your body producing too many red blood cells in response to testosterone — is the single most common dose-limiting adverse effect of TRT. It does not make headlines the way "heart attacks" do, but it affects far more patients.
In a 20-year longitudinal cohort of 1,073 people on testosterone, the probability of developing erythrocytosis reached 10% at one year and 38% by ten years of treatment (Madsen et al., 2021). In a single-center retrospective study of 247 TRT patients (median follow-up 2.9 years), 57% reached a hematocrit above 0.46, 23% exceeded 0.50, and 5% crossed 0.54 — the clinical threshold where intervention is required (Neidhart et al., 2024).
The guideline discontinuation threshold is hematocrit 54%. That figure comes from FDA labeling and is backed by clinical consensus (Chin-Yee et al., 2017). Above that level, you either dose-reduce, switch formulations, or stop therapy temporarily.
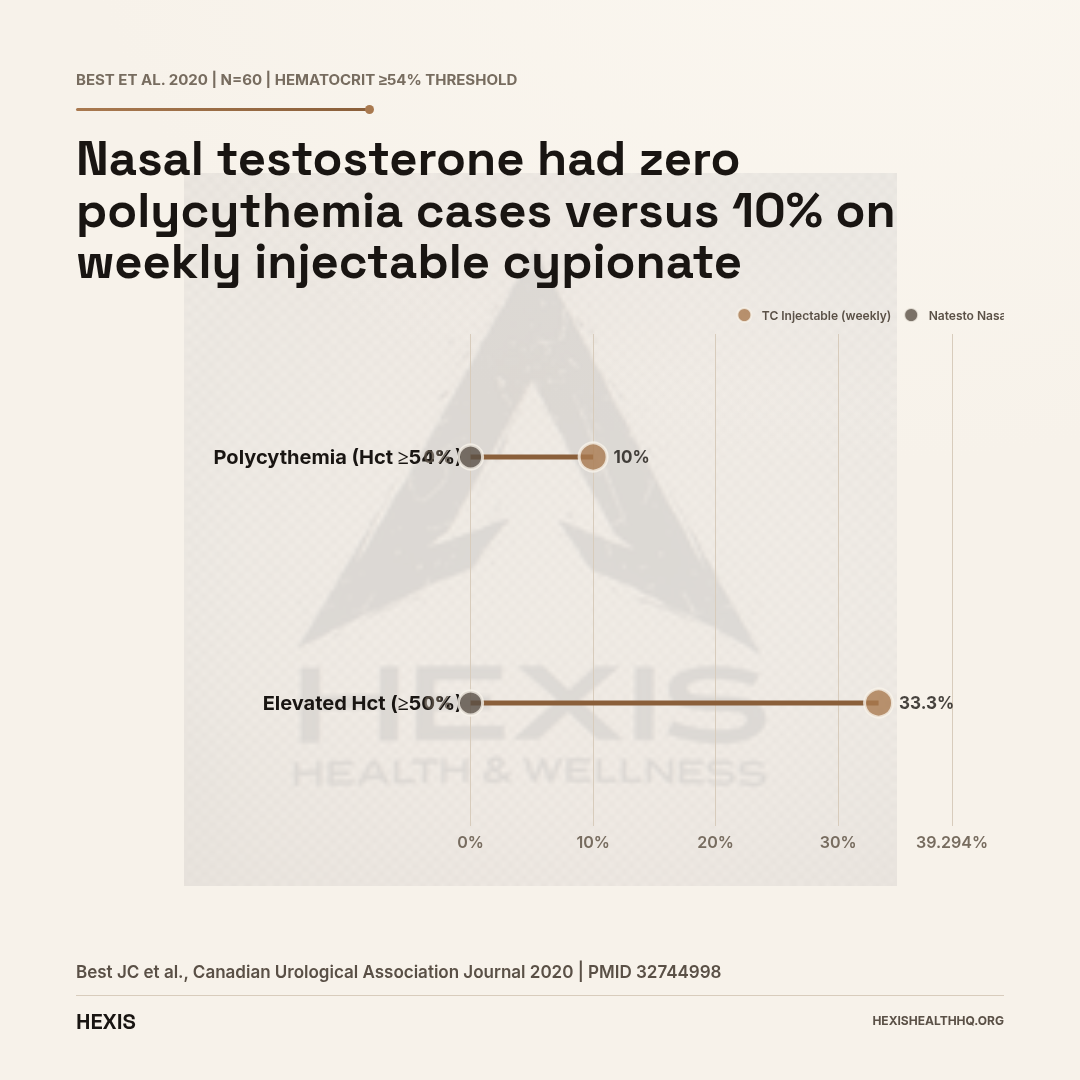
Formulation matters — a lot. Long-acting testosterone undecanoate carried an odds ratio of 2.9 (95% CI 1.7–5.0) for erythrocytosis versus shorter-acting formulations (Madsen et al., 2021). A direct comparison of testosterone cypionate IM versus Natesto (nasal gel) in 60 patients found polycythemia (Hct ≥54%) in 10% of the cypionate group and 0% in the Natesto group (Best et al., 2020). Injectable testosterone cypionate raised hematocrit by 3.24 percentage points on multivariable regression.
If your hematocrit keeps climbing on injections, switching to a lower-peak formulation is a legitimate clinical strategy — not a downgrade.
Gynecomastia and Elevated Estradiol
Gynecomastia and elevated estradiol are real TRT side effects — most common in men on injectable formulations and those with higher body fat, where aromatization (testosterone converting to estradiol in adipose tissue) runs highest. That conversion is normal physiology; the problem is when it outpaces what your body needs.
A screening review of 34,016 men presenting to Low T Centers found that hyperestrogenism and gynecomastia were documented adverse effects, particularly among those converted to injectable TRT (Tan et al., 2014). Symptoms range from mildly tender nipples to actual breast tissue growth.
Estradiol itself is not the enemy — men need it for bone density, libido, and mood. The issue is when it climbs high enough to stimulate breast tissue. Some men never get there; others get there at testosterone levels that would never trigger symptoms in someone with lower adiposity.
Aromatase inhibitors are used off-label to manage high estradiol in TRT patients. That's a clinical decision, not a DIY one — crashing estradiol too low causes its own problems (joint pain, low libido, poor sleep).
Testicular Atrophy and Fertility
TRT suppresses the hypothalamic-pituitary-gonadal (HPG) axis, causing testicular atrophy and reduced sperm production in essentially all men who use it — the degree varies, but some level of testicular volume loss and fertility impact is expected, not the exception.
Exogenous testosterone signals the brain that enough is circulating. Your brain stops sending LH and FSH signals to the testes because it sees plenty of testosterone in circulation. Without that signal, intratesticular testosterone production drops — and so does sperm production. The result: testicles that are smaller than before, and sperm counts that range from significantly reduced to zero.
This is not a rare effect. It's an expected physiological consequence of HPG suppression — it happens to some degree in essentially everyone on TRT.
For men who want to father children, TRT without fertility protection is a problem. Options exist — hCG co-administration can preserve intratesticular testosterone production and maintain sperm production, and Natesto's nasal delivery mechanism produces lower HPG suppression than systemic formulations. If fertility is a priority, those options need to be part of the conversation before starting TRT, not after.
For a full breakdown of fertility management on TRT, see our dedicated guide: TRT and fertility: what the research says.
“TRT was not associated with increased high-grade prostate cancer risk compared with placebo — in the same 5,246-man cohort that tested cardiovascular safety.”
Does TRT Cause Prostate Cancer?
No — and this has now been studied directly in a large randomized trial.
The TRAVERSE prostate substudy enrolled the same 5,246-man cohort and tracked prostate safety events prospectively. TRT was not associated with increased high-grade prostate cancer risk compared with placebo (Bhasin et al., 2023). The RHYME registry followed 999 hypogonadal men (750 on TRT, 249 untreated) and found TRT was not associated with increased prostate cancer risk either (Debruyne et al., 2017).
The historical concern traced back to the Huggins era — if removing androgens shrank prostate cancers, the thinking went, testosterone must promote them. That logic made sense in the 1940s. It hasn't held up in prospective randomized data.
What TRT does do is raise PSA — prostate-specific antigen — because PSA is an androgen-sensitive protein. That PSA rise needs to be monitored, and TRT is contraindicated in men with known or suspected prostate cancer. The TRAVERSE trial excluded any man with a baseline PSA above 3.0 ng/mL without prior urology evaluation.
PSA monitoring is standard of care on TRT — not because TRT causes cancer, but because cancer monitoring needs to continue regardless of what you're on.
Sleep Apnea
TRT can worsen pre-existing obstructive sleep apnea (OSA), and it may unmask OSA in men who have undiagnosed mild disease. This was noted as far back as 1978 in a case report showing worsened nighttime apneas, and the FDA has carried a label warning on it ever since (Payne et al., 2020).
The mechanism likely involves testosterone's effects on upper airway muscle tone and ventilatory drive. Men with untreated moderate-to-severe OSA should have CPAP in place before starting TRT, or the combination can significantly worsen sleep quality and oxygen saturation — negating some of the energy benefits people start TRT for in the first place.
If you've been told you snore heavily or wake up unrefreshed, get an OSA screen before starting.
What Does TRT Do to Your Skin?
Testosterone is androgenic, which means acne and oily skin are real possibilities — particularly in men who were acne-prone before starting. This is the same mechanism as puberty-related acne, just triggered later.
The dermatological adverse effect profile of TRT spans acne, seborrhea, hair thinning (in men with genetic predisposition), and at injection sites: local reactions including pain, bruising, and erythema. A scoping review confirmed these patterns across formulations, with injectable and topical formulations having distinct dermatological profiles (Abou Chawareb et al., 2026).
None of these are reasons to avoid TRT if it's otherwise indicated — but they're worth knowing about before you start, not after.
What Labs Do You Need on TRT, and How Often?
Five parameters require scheduled monitoring on TRT: hematocrit, PSA, testosterone levels, lipids, and sleep apnea screening. The calendar below reflects FDA labeling and current clinical practice — skipping any of these is where manageable effects become unmanaged ones.
| Parameter | Baseline | 3–6 Months | Annually |
|---|---|---|---|
| Hematocrit | Yes | Yes | Yes |
| PSA | Yes | Yes | Per AUA guidelines |
| Total testosterone | Yes | Yes (trough/mid-cycle) | Yes |
| Lipid panel | Yes | — | As indicated |
| Sleep apnea screen | Yes | — | — |
Hematocrit: Check at baseline, 3–6 months, and then annually. If it hits 54%, the protocol is to reduce dose, switch to a lower-peak formulation, or pause therapy.
PSA: Baseline before starting. Recheck at 3–6 months. Any rise of more than 1.4 ng/mL in any 12-month period, or a PSA above 4.0 ng/mL, warrants urology referral.
Testosterone levels: For injectable testosterone, check trough (day before injection). For gels, check mid-cycle. Target range is typically 400–700 ng/dL.
TRT is a DEA Schedule III controlled substance and requires documented hypogonadism — two morning testosterone concentrations below 300 ng/dL, plus symptoms — to prescribe legally. It's not approved for anti-aging or performance enhancement. Athletes should also know that testosterone is on the WADA S1.1 prohibited list at all times; a Therapeutic Use Exemption (TUE) is available for documented hypogonadism.
If you want to understand the full range of treatment approaches for low testosterone before deciding whether TRT is right for you, our guide to how to treat low testosterone covers the decision framework in detail.
Erythrocytosis Risk by Formulation
Polycythemia rate and hematocrit elevation by delivery method
| Testosterone Cypionate IM | Natesto Nasal Gel | |
|---|---|---|
| Polycythemia (Hct ≥54%) | 10% | 0% |
| Hct ≥50% | 33.3% | 0% |
| Hct increase (regression) | +3.24 pts | Minimal |
| HPG axis suppression | Full | Partial |
| Dosing frequency | Weekly | 3× daily |
Source: Kohn TP et al., Journal of Sexual Medicine, 2020 (PMID 32744998)
Injectable vs. Gel: Does the Delivery Method Change the Risk Profile?
Injectable testosterone carries meaningfully higher erythrocytosis and estradiol-conversion risk than gels or nasal formulations — driven by peak concentration differences, not the hormone itself.
Erythrocytosis risk is higher with injectable formulations, particularly testosterone cypionate given weekly (Best et al., 2020). The higher peak concentrations with IM injections drive more red blood cell stimulation than the flatter concentration curve of daily gels.
Estradiol conversion also runs higher with injectables, for the same peak-concentration reason. Men who are prone to gynecomastia or high estradiol on injections sometimes do better converting to a gel or nasal formulation.
Natesto (nasal testosterone gel) is in a category of its own — it has the lowest erythrocytosis rate of any available formulation (0% at Hct ≥50% in one head-to-head study) and produces less HPG suppression, which preserves more fertility potential. The tradeoff is three-times-daily dosing and a significant rate of nasal irritation.
For a full comparison of injection protocols, concentration curves, and formulation-specific considerations, see our guide to injectable testosterone.
Frequently Asked Questions
Is testosterone replacement therapy safe for your heart?
Based on TRAVERSE — the largest RCT ever conducted on this question, with 5,246 men — TRT did not increase MACE (heart attack, stroke, cardiovascular death) versus placebo (Lincoff et al., 2023). There were signals for atrial fibrillation (3.5% vs. 2.4%) and pulmonary embolism (0.9% vs. 0.5%). For most men with documented hypogonadism, the cardiac risk profile is acceptable with proper monitoring.
What hematocrit level is too high on TRT?
The guideline threshold is 54%. Above that, current FDA labeling and clinical practice call for dose reduction, formulation switch, or a treatment pause (Chin-Yee et al., 2017). Routine hematocrit checks at baseline, 3–6 months, and annually are standard of care on TRT.
Does TRT cause prostate cancer?
No — the TRAVERSE prostate substudy found no increase in high-grade prostate cancer risk with TRT versus placebo in a 5,246-man RCT (Bhasin et al., 2023). TRT does raise PSA because PSA is androgen-sensitive, which is why PSA monitoring is part of the standard protocol — not because TRT causes cancer.
Will TRT make my sleep apnea worse?
It can. TRT may worsen pre-existing obstructive sleep apnea by affecting upper airway tone and ventilatory drive (Payne et al., 2020). Screening for OSA before starting TRT is standard. If you have untreated moderate-to-severe OSA, get CPAP in place first.
Can I have children while on TRT?
Standard TRT suppresses the HPG axis and reduces or eliminates sperm production. This is expected, not rare. If fertility matters to you, discuss hCG co-administration or nasal testosterone (Natesto) before starting — not after. For the full picture, read our guide to TRT and fertility.
Starting TRT With the Right Support
Every major TRT side effect in this article has a monitoring checkpoint that catches it before it becomes a clinical problem — that's not reassurance, it's what the protocol is designed to do.
TRT goes wrong when it happens without those guardrails — prescribed without baseline labs, run without follow-up, sourced outside a supervised medical context. That's when side effects stop being data points and start being emergencies.
At HEXIS, every TRT protocol starts with a full hormone panel, hematocrit, PSA, and lipids before a single prescription is written. Monitoring is built into the protocol, not added later. If you want to know whether TRT makes sense for your situation, schedule a consultation and we will start with your numbers.
TRT Side Effects & Safety: The Bottom Line
- 1
The TRAVERSE trial (n=5,246) confirmed TRT does not increase major cardiac events versus placebo — AFib (3.5% vs 2.4%) and PE (0.9% vs 0.5%) signals are real but did not cancel the noninferiority finding.
- 2
Erythrocytosis is the most common dose-limiting effect, with 38% cumulative risk at 10 years — and it is formulation-dependent, with injectable testosterone driving far more hematocrit elevation than nasal or gel delivery.
- 3
Every risk on this list is manageable with the right monitoring in place: hematocrit, PSA, testosterone levels, and a sleep apnea screen before starting — that is the protocol that makes TRT safe.