Types of Testosterone & Delivery Methods: A Complete Clinical Guide
Types of Testosterone & Delivery Methods
Not all testosterone is the same — and not all ways to deliver it produce the same result in your body. There are currently seven distinct delivery routes approved for clinical use, each with its own pharmacokinetics, dosing schedule, and trade-offs. What works well for one person may be a poor fit for another, and the differences matter more than most prescribers take time to explain.
The short answer: Testosterone replacement therapy comes in injectable esters (cypionate, enanthate), long-acting injectable undecanoate (Nebido/Aveed), transdermal gels (AndroGel, Testim), transdermal patches (Androderm), oral undecanoate capsules (Jatenzo, Kyzatrex), nasal gel (Natesto), and subcutaneous pellets (Testopel). Each route differs in how quickly levels peak, how stable they stay, and how often you need a dose.
This article covers all seven routes — their pharmacokinetics, clinical efficacy data, and the trade-offs you should understand before choosing one. For deep dives on specific formulations, see the sibling articles on injectable testosterone, AndroGel, Jatenzo, and Natesto.
How Does Testosterone Get Into Your Bloodstream?
The delivery route determines almost everything: how fast testosterone levels rise, how high they peak, how long they stay in range, and what side effects become more or less likely. This is pharmacokinetics — and it's the single biggest factor separating one formulation from another.
Testosterone is a lipophilic steroid. When you inject an oily ester solution into muscle or fat tissue, the ester is slowly cleaved from the testosterone molecule as it diffuses out of the depot — controlling release rate. When you apply a gel to skin, testosterone diffuses through the stratum corneum and into circulation continuously. Oral forms bypass the liver differently than the old methyltestosterone (which was liver-toxic) by absorbing through intestinal lymphatics rather than portal circulation.
The key metric for comparing formulations is the peak-to-trough ratio — how far levels swing between their highest and lowest point in a dosing cycle. A high ratio means supraphysiological peaks followed by sub-normal troughs. A flat ratio means levels stay closer to a consistent physiological range the whole time.
Injectable Testosterone Esters: Cypionate and Enanthate
Injectable testosterone cypionate (TC) and enanthate (TE) are the most prescribed forms of TRT in the United States — and for most hypogonadal men, they remain the right starting point: cost-effective, well-studied, and appropriate as initial therapy (Campbell et al., 2023).
Both TC and TE are typically injected intramuscularly (IM) every 1–2 weeks at clinic, or weekly via self-injection, though subcutaneous (SC) administration is increasingly common. A population PK model of depot TC estimated a mean clearance of 2.6 kL/day and a volume of distribution of 14.4 kL — parameters that vary with body weight and albumin levels (Bi et al., 2018).
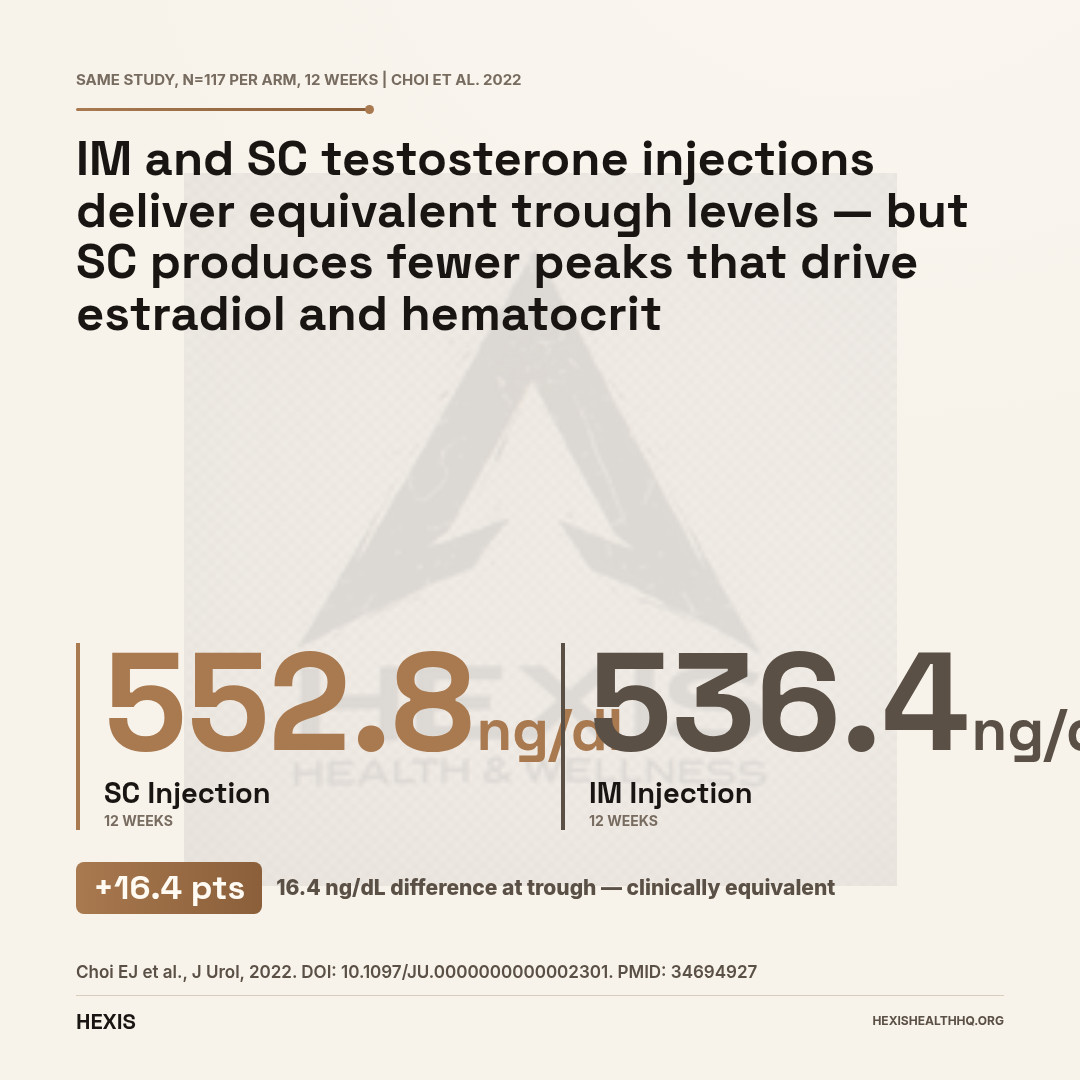
The clinical trade-off is the peak-to-trough swing. In a direct comparison study, men on IM testosterone cypionate 100 mg weekly saw trough total testosterone rise from a mean of 313.6 ng/dL at baseline to 536.4 ng/dL at 12 weeks — a meaningful gain. Their counterparts on a subcutaneous testosterone enanthate autoinjector (SCTE-AI) went from 246.6 ng/dL to 552.8 ng/dL (Choi et al., 2022). Trough levels were statistically equivalent, but the IM group had higher post-therapy estradiol and hematocrit — a consequence of supraphysiological peaks driving more aromatization and erythropoiesis.
For a detailed breakdown of cypionate versus enanthate — half-life, ester weight, dosing protocols — see testosterone enanthate vs cypionate.
Subcutaneous Injection: The Better Route for Most People
Subcutaneous (SC) testosterone injection produces equivalent testosterone exposure to intramuscular injection — with meaningfully better tolerability. In a crossover study of 14 participants, SC and IM injections of TC and TE produced equivalent dose-normalized AUC (1.7 vs. 1.9 nmol·days/L/mg; p > 0.05), but SC participants reported lower pre-injection anxiety, less pain during, and less soreness after (Wilson et al., 2018).
A separate study of weekly SC testosterone cypionate in 11 patients documented a mean total testosterone of 627 ng/dL between injections, with stable levels across the dosing interval (McFarland et al., 2017). SC injections are also easy to self-administer — smaller needle, abdomen or thigh, no clinic visit required.
The Choi et al., 2022 comparison (n = 234) added an important safety dimension: SCTE-AI was independently associated with lower post-therapy estradiol and lower hematocrit versus IM-TC, even after controlling for confounders. Less peak-driven aromatization. Lower erythrocytosis risk. The pharmacokinetics are the explanation — a flatter curve means less conversion.
Long-Acting Injectable Testosterone Undecanoate (Nebido / Aveed)
Injectable testosterone undecanoate (TU) — marketed as Nebido outside the US and Aveed in the US — enables dosing every 10–12 weeks, compared to every 1–2 weeks for standard esters. That interval is possible because TU dissolves in castor oil, which creates a slow-release depot with a terminal half-life of 33.9 days — roughly 7 times longer than testosterone enanthate (Behre et al., 1999).
In the original phase I dose-finding study (n = 14), all participants maintained testosterone in the eugonadal range between doses, with no supraphysiological peaks — a sharp contrast to the weekly-injection profile of TC and TE (Behre et al., 1999). That flat PK curve is what makes the extended interval clinically workable.
The benefit: no weekly injections, stable levels over a 3-month window, and strong compliance data from long-term observational cohorts. A 12-year observational study of elderly and younger patients receiving quarterly TU injections showed sustained eugonadal testosterone levels with manageable hematocrit increases — and no significant between-group differences in adverse events by age (Abildgaard et al., 2022).
The downside is that it requires office administration in the US due to a post-injection observation period (risk of pulmonary oil microembolism), involves a large injection volume, and cannot be quickly adjusted if levels are too high or too low.
Do Transdermal Gels and Patches Produce Steadier Levels Than Injections?
Transdermal delivery — gels and patches — achieves something injectable esters struggle with: consistent, near-physiological testosterone levels without peaks and troughs. The short answer is yes, and there is systematic review evidence to back it.
A systematic review of testosterone therapy formulations found that transdermal gels and long-acting injectable TU are the two formulations that most reliably achieve steady-state levels within the physiological range (Al-Zoubi et al., 2021). That finding matters because stable levels translate to more stable mood, energy, and libido — and less erythrocytosis risk from repeated supraphysiological spikes.
Transdermal Gels (AndroGel, Testim, Vogelxo)
Gels are applied daily to the shoulders, upper arms, or abdomen. Absorption is continuous and relatively predictable, though there is meaningful inter-individual variability — some men absorb efficiently, some do not, and levels need to be checked 2–4 hours post-application (the absorption peak) for accurate monitoring.
Transfer to partners or children via skin-to-skin contact is a real concern with gels and requires specific precautions — covering the application site, washing hands, and avoiding contact before the gel dries. This is not a theoretical risk; FDA labeling includes warnings based on reported virilization events in children.
For application technique, dosing titration, and the full safety profile, see AndroGel and testosterone gels.
Transdermal Patches (Androderm)
Patches deliver testosterone through a membrane-controlled reservoir applied daily, typically to the back, abdomen, or thigh. They produce stable levels similar to gels. The primary clinical limitation is skin irritation — patch-site reactions occur in a substantial proportion of users, and that tends to be the main reason men switch formulations.
Oral TU raises blood pressure — monitor before and during treatment
Two years of Jatenzo treatment was associated with a 3–6 mmHg increase in systolic blood pressure and a –9.8 mg/dL decrease in HDL cholesterol. The newer Kyzatrex formulation showed a smaller signal: +1.7 mmHg (95% CI 0.3–3.1) on 24-hour ambulatory monitoring.
Patients with borderline hypertension or existing cardiovascular risk factors should have blood pressure and lipids monitored before starting and at each follow-up visit.
Source: Honig et al., J Sex Med, 2022; Bernstein & Dhingra, Ther Adv Urol, 2024
Oral Testosterone Undecanoate: Jatenzo, Kyzatrex, and Tlando
Oral testosterone has a complicated history. The old 17-alpha-alkylated oral androgens (methyltestosterone) caused liver toxicity because they were designed to resist first-pass hepatic metabolism. Testosterone undecanoate takes a completely different route: it absorbs through intestinal lymphatics, bypassing the liver almost entirely. No liver toxicity signal has been found in trials extending out to two years (Swerdloff & Dudley, 2020).
The efficacy data is solid. In the pivotal Jatenzo phase III trial, 87% of hypogonadal men achieved a mean T Cavg in the eugonadal range — the same percentage as the topical testosterone comparator arm. Mean plasma T Cavg was 403 ng/dL (serum equivalent ~489 ng/dL) over 3–4 months (Swerdloff et al., 2020). A one-year extension trial reported 84% eugonadal achievement and a serum T Cavg of 628 ng/dL (Swerdloff & Dudley, 2020). At two years of continuous treatment, testosterone levels remained in eugonadal range in 69 men who completed the extension (Honig et al., 2022).
Kyzatrex, the newer oral TU formulation, produced eugonadal T in 87.8% of participants in a phase III trial, with a mean serum Cavg of 452 ng/dL at 90 days (Bernstein & Dhingra, 2024).
The Fat Dependency of Oral TU — This Actually Matters
Oral TU absorption is almost entirely fat-dependent. The mechanism: dietary fat stimulates lymphatic transport in the gut, which is the pathway oral TU uses to enter circulation. Without adequate dietary fat, absorption collapses.
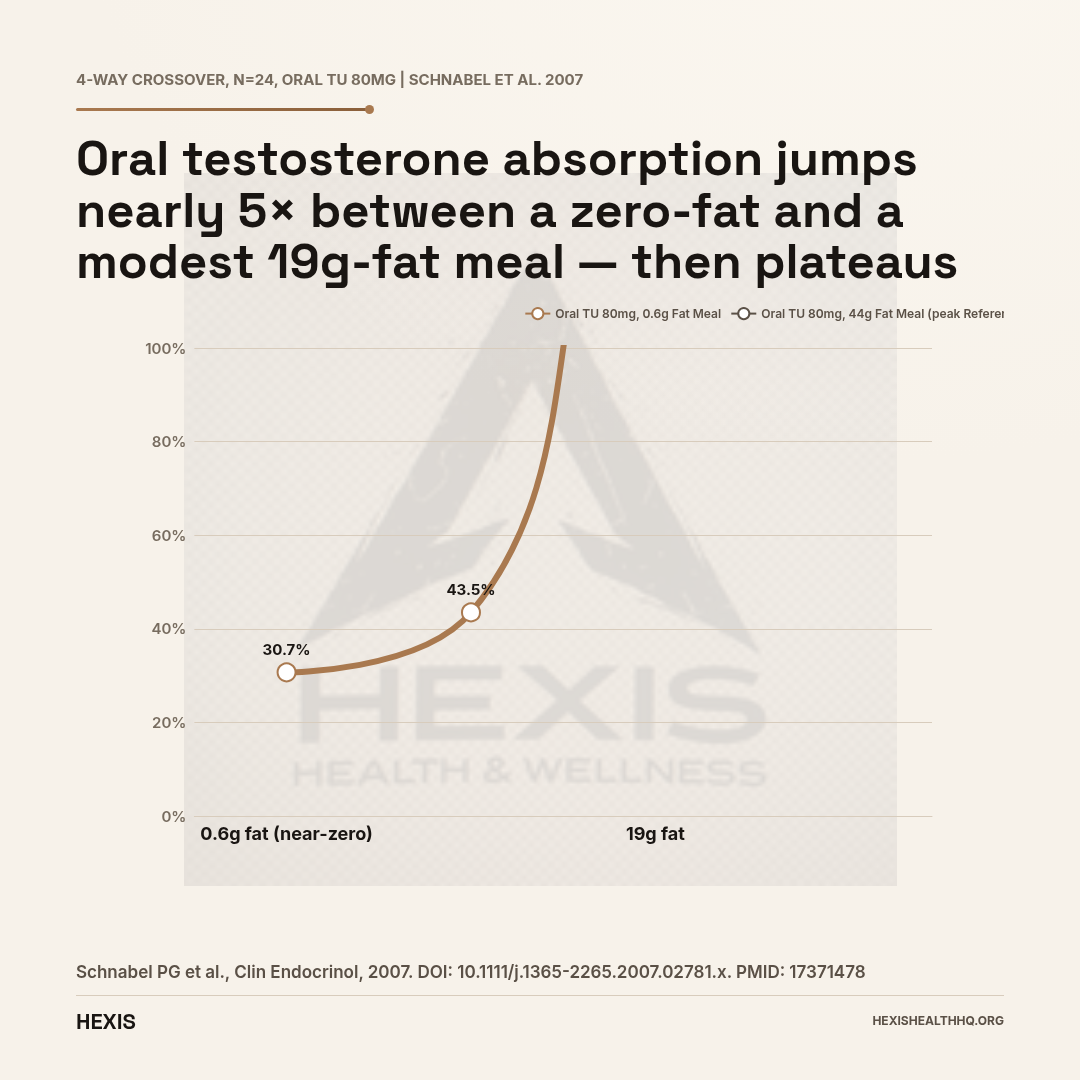
The numbers are stark. In a four-way crossover study, men who took oral TU with a near-zero fat meal (0.6 g lipid) had an AUC of 30.7 nmol·h/L. The same dose taken with a meal containing just 19 g of fat (roughly two eggs and a small amount of olive oil) produced an AUC of 146 nmol·h/L — a nearly five-fold difference (Schnabel et al., 2007). Increasing fat further to 44 g raised the AUC only marginally to 154 nmol·h/L. The practical takeaway: you do not need a fatty meal, but you need a meal with some fat — skipping the fat altogether essentially means skipping the dose.
Blood Pressure: The Signal Worth Understanding
All oral TU trials show a modest systolic blood pressure increase. In the Jatenzo trials, systolic BP rose by 3–6 mmHg (Honig et al., 2022). In the Kyzatrex trial, 24-hour ambulatory systolic BP increased by 1.7 mmHg (95% CI 0.3–3.1) — a smaller signal (Bernstein & Dhingra, 2024). The HDL cholesterol effect is also real: Jatenzo was associated with a –9.8 mg/dL decrease in HDL at two years (Honig et al., 2022). These are not reasons to avoid oral TU, but they are reasons to monitor blood pressure and lipids — as you should with any TRT.
For dosing schedules, titration protocols, and the full Jatenzo prescribing profile, see Jatenzo oral testosterone.
87.0% relative scale
of hypogonadal men achieved eugonadal testosterone levels on oral TU (Jatenzo) — the same rate as topical testosterone in the same trial (Swerdloff et al., 2020)
Nasal Testosterone Gel (Natesto): The Fertility-Preserving Option
Natesto is testosterone gel applied intranasally — 11 mg per dose, three times daily (TID). It sounds inconvenient, but its pharmacological profile is unique in a meaningful way.
Because each dose is small and cleared quickly, Natesto produces brief, pulsatile testosterone peaks rather than the sustained suppression of the hypothalamic-pituitary-gonadal (HPG) axis that characterizes other TRT routes. In a study examining the spermatogenesis effects of different TRT formulations, nasal testosterone preserved luteinizing hormone (LH) pulses and spermatogenesis in men who would have been suppressed on injectable or transdermal therapy (Campbell et al., 2023).
Hypogonadal men who want to maintain fertility while treating testosterone deficiency have exactly one approved TRT option that won't shut down sperm production. Every other route suppresses the HPG axis. Natesto is the only FDA-approved testosterone therapy with evidence for preserved spermatogenesis.
For the complete fertility data and the practical protocol, see Natesto nasal testosterone gel.
How Long Do Testosterone Pellets (Testopel) Actually Last?
Testosterone pellets last approximately 4–5 months per implantation — longer than any other self-contained delivery method. They are small, crystalline testosterone cylinders — typically 75 mg each — inserted subcutaneously in the upper buttock under local anesthesia. The procedure takes under 10 minutes and is done in-office. Testosterone is released slowly as the pellet is resorbed.
In the original characterization study, six hypogonadal men implanted with 6 × 100 mg pellets (600 mg total) maintained a mean serum testosterone of 17 nmol/L over 21 weeks — a duration lower bound of approximately 4 months (Cantrill et al., 1984). Levels stay in range for roughly 4–5 months before another implantation is needed.
Pellets are attractive for patients who want to avoid frequent dosing. You get implanted, levels stabilize, and you come back in 4–5 months. No daily applications. No weekly shots. The downsides: office visits for every implantation, a minor surgical procedure each time, risk of pellet extrusion (~4% of insertions), and no easy dose adjustment if levels run high — you cannot "take out" a pellet once it is in.
Patient preference data adds nuance. In a randomized crossover study comparing injectable TU to subcutaneous pellet implants, 91% of men preferred injectable TU over pellets at study end (Fennell et al., 2010). The preference driver was primarily the procedure requirement — men found the quarterly injection preferable to the subcutaneous insertion.
Buccal Testosterone (Striant)
Buccal testosterone (Striant) delivers testosterone through the gum mucosa rather than the skin or muscle — a twice-daily adhesive tablet pressed against the gum above the upper incisor. It produces stable serum testosterone levels without the skin-contact transfer risk associated with topical gels, because absorption occurs locally through the buccal membrane rather than across exposed skin.
The primary limitation is local tolerability. Gum irritation and mouth discomfort from the adhesive pad are the most commonly reported complaints, and twice-daily dosing is a compliance barrier compared to weekly injections or daily gel. Striant fills a specific niche: patients who cannot use transdermal formulations (skin conditions, contact-transfer risk with children or partners) and who are averse to injection. It is rarely the starting point for a new TRT patient.
Testosterone Delivery Routes: Side-by-Side
Peak-to-trough ratio and dosing frequency by formulation
| Route | Dosing Frequency | Peak-to-Trough | Key Study |
|---|---|---|---|
| IM ester (TC/TE) | Weekly | High | Choi et al., 2022 |
| SC ester (autoinjector) | Weekly | Moderate | Wilson et al., 2018 |
| Injectable TU (Nebido/Aveed) | Every 10–12 wk | Low | Behre et al., 1999 |
| Transdermal gel | Daily | Very low | Al-Zoubi et al., 2021 |
| Transdermal patch | Daily | Very low | — |
| Oral TU (Jatenzo/Kyzatrex) | Twice daily | Low–moderate | Swerdloff et al., 2020 |
| Nasal gel (Natesto) | 3× daily | Very low | Campbell et al., 2023 |
| Pellets (Testopel) | Every 4–5 months | Very low | Cantrill et al., 1984 |
| Buccal (Striant) | Twice daily | Low | — |
Source: Choi 2022 (PMID 34694927), Behre 1999 (PMID 10229906), Swerdloff 2020 (PMID 32382745), Al-Zoubi 2021 (PMID 34552788)
Comparing the Routes: What the Data Actually Shows
| Route | Dosing Frequency | Peak-to-Trough | Key Evidence |
|---|---|---|---|
| IM ester (TC/TE) | Weekly | High | Choi et al., 2022 |
| SC ester | Weekly | Moderate | Wilson et al., 2018 |
| Injectable TU | Every 10–12 wk | Low | Behre et al., 1999 |
| Transdermal gel | Daily | Very low | Al-Zoubi et al., 2021 |
| Transdermal patch | Daily | Very low | — |
| Oral TU | Twice daily | Low–moderate | Swerdloff et al., 2020 |
| Nasal gel | Three times daily | Very low | Campbell et al., 2023 |
| Pellets | Every 4–5 months | Very low | Cantrill et al., 1984 |
| Buccal | Twice daily | Low | — |
No single route is objectively best. The right choice depends on your preferences for dosing frequency, tolerance for injection procedures, fertility goals, blood pressure baseline, and whether you want clinic-based or self-managed administration.
What Determines Which Route Is Right?
No single answer fits everyone. What shifts the decision is a combination of your clinical situation and your life.
Fertility preservation is the clearest determinant. If you want to maintain sperm production, nasal testosterone (Natesto) is the only approved TRT option with evidence for preserved spermatogenesis (Campbell et al., 2023). Every other route suppresses the HPG axis — that's not debatable.
Dosing frequency matters more than patients expect. Long-acting injectable TU (every 10–12 weeks) and pellets (every 4–5 months) minimize the frequency of intervention. But daily gels and patches require consistency, and three-times-daily nasal dosing is a real compliance ask.
Peak-to-trough dynamics affect your side effect profile. High-peak formulations — weekly IM injections — drive more estradiol conversion and hematocrit elevation. If your hematocrit is already borderline or your E2 tends to run high, a flatter formulation like a gel, SC injection, or long-acting injectable will typically produce a cleaner profile.
Blood pressure baseline is relevant if you're considering oral TU. The 1.7–6 mmHg systolic increase documented across trials is modest, but it's real. In patients with borderline hypertension or existing cardiovascular risk, that signal shifts the math toward a different route.
Needle or skin aversion is practical, not trivial. Gels and patches avoid needles entirely. Natesto avoids both needles and skin application. But patches cause skin irritation in a meaningful minority of users, and intranasal dosing three times daily isn't frictionless either.
Cost often makes the decision by default. Injectable cypionate and enanthate remain the most cost-effective options and are appropriate as first-line therapy for most men (Campbell et al., 2023). Oral TU formulations and Natesto carry significantly higher out-of-pocket costs.
Getting Started With Testosterone Replacement Therapy
The selection process starts with accurate labs — not a questionnaire, not a symptom checklist alone. You need morning total testosterone (ideally drawn twice, 2 weeks apart), free testosterone, LH, FSH, estradiol, complete blood count, and a metabolic panel. These numbers together tell your provider what is happening hormonally and what baseline safety parameters to monitor once you start a formulation.
At HEXIS, every TRT protocol is managed by licensed medical providers — physicians and nurse practitioners with specific training in hormone replacement. Every protocol starts with a full panel. We don't prescribe based on symptoms alone, and we don't recommend a specific formulation without knowing your cardiovascular risk factors, fertility goals, and lifestyle. That information shapes the delivery route decision more than any single clinical metric.
If you're ready to have that conversation, schedule a consultation and we'll build a protocol around your actual numbers.
Frequently Asked Questions
Which type of testosterone is the most effective?
Effectiveness is route-neutral — what matters is whether your levels land consistently in the eugonadal range (300–1000 ng/dL). Injectable esters, oral TU, transdermal gels, and long-acting injectable TU have all demonstrated 84–87% eugonadal achievement rates in clinical trials. The best type is the one you will use consistently and that fits your clinical profile.
Does the delivery method affect testosterone side effects?
Yes, meaningfully. High-peak formulations like IM weekly injections drive more estradiol conversion and hematocrit elevation than flat-curve options like gels or subcutaneous injections. Oral TU adds a modest blood pressure signal (1.7–6 mmHg systolic). Nasal testosterone is the only route with evidence for preserved fertility.
Can I switch testosterone delivery methods?
Yes. Switching formulations is common as patient needs change. The transition typically involves a washout period or overlap depending on the half-lives involved. Any switch requires re-titration — your provider will recheck levels 4–6 weeks after the new formulation is established to confirm you are in range.
Is oral testosterone bad for your liver?
Modern oral testosterone undecanoate (Jatenzo, Kyzatrex, Tlando) is not liver-toxic. It absorbs through intestinal lymphatics, bypassing the liver's first-pass metabolism. Two-year trial data showed no clinically significant changes in liver function tests (Honig et al., 2022). The concern about liver toxicity applies to the old 17-alpha-alkylated oral androgens (methyltestosterone), which are no longer used in legitimate TRT.
How long does it take to see results from testosterone therapy?
The timeline depends on the formulation and what you are measuring. Energy and libido often improve within 3–6 weeks. Body composition changes (lean mass, fat reduction) require 3–6 months of consistent therapy to become measurable. Bone density improvements take 12+ months. The Swerdloff & Dudley, 2020 one-year trial showed +3.2 kg lean mass and –2.4 kg fat mass at 365 days — those are real but not rapid changes.
Types of Testosterone & Delivery Methods: The Bottom Line
- 1
No single formulation is best — the right route depends on fertility goals, dosing tolerance, cardiovascular baseline, and cost. Injectable cypionate and enanthate remain first-line for most men because they are effective and cost-efficient (Campbell et al., 2023).
- 2
Pharmacokinetics drive the side effect profile. High-peak formulations (weekly IM injections) elevate estradiol and hematocrit more than flat-curve options like transdermal gels or subcutaneous injections. If those lab values matter for you, the route choice matters.
- 3
Natesto is the only approved TRT option with evidence for preserved spermatogenesis. If fertility is a priority, it's the conversation to have with your provider before starting any other form of testosterone replacement.