Does Low Testosterone Cause Weight Gain?
Does Low Testosterone Cause Weight Gain?
You're eating the same food. You're still getting to the gym most weeks. But your belt is on a different notch than it was two years ago, and nothing you try seems to move it back. If you're a man in your 40s or 50s, this question has probably crossed your mind: does low testosterone cause weight gain — or is this just aging?
The honest answer is yes, low testosterone contributes to fat gain. But the more important answer is that the relationship runs in both directions. Low testosterone promotes fat accumulation, and fat accumulation drives testosterone even lower. Once you're in that loop, it's hard to break — and most standard medical advice doesn't address both sides of it.
The short answer: Low testosterone promotes visceral fat accumulation and loss of muscle mass. A large cohort study (n=3.49 million) found men with low testosterone had an 89% higher risk of type 2 diabetes (Saffati et al., 2026). Testosterone replacement therapy reduced body weight by an average of 3.91 kg and waist circumference by 2.8 cm in a meta-analysis of 18 clinical trials (Li et al., 2020). TRT is body recomposition — not a simple weight-loss drug — and it works best combined with exercise.
What Testosterone Actually Does to Your Body Composition
Testosterone directly regulates muscle protein synthesis, fat cell activity, and energy metabolism — which is why a drop in T affects how your body looks and performs even before you notice it on the scale.
In muscle, testosterone binds to androgen receptors and triggers protein synthesis — it's one of the main signals telling your body to build and maintain lean mass. When T drops, that signal weakens. You lose muscle more easily and rebuild it more slowly after training.
In fat tissue, testosterone suppresses lipid uptake and promotes fat breakdown. Low testosterone removes that brake — fat cells, especially visceral fat (the dangerous kind that wraps around your organs), become more metabolically active at storing energy.
The combined effect: lower lean mass, higher fat mass, slower metabolism. Even if you haven't changed what you eat or how much you exercise, your body composition can drift in the wrong direction when testosterone falls below a functional threshold.
This is supported by the clinical data. A 2015 review of testosterone's direct effects on adipose tissue found that testosterone inhibits fat cell differentiation, reduces lipid uptake, and promotes lipolysis — the breakdown of stored fat (Kelly & Jones, 2015).
The Bidirectional Cycle: How Low T and Fat Feed Each Other
Fat causes low testosterone just as surely as low testosterone causes fat gain — and the mechanism running between them is specific, measurable, and reversible. Most articles about low T and weight don't explain this half of the equation.
Visceral fat — the fat packed around your abdominal organs — is metabolically active. It contains high concentrations of an enzyme called aromatase. Aromatase converts testosterone into estradiol (a form of estrogen). The more visceral fat you carry, the more of your testosterone gets converted before it can do its job.
High estradiol, in turn, signals the hypothalamic-pituitary-gonadal (HPG) axis — the hormonal command chain that controls testosterone production — to reduce output. Your brain reads the elevated estradiol as a sign that testosterone is sufficient, so it dials back production.
That's the loop: visceral fat raises aromatase activity, which lowers free testosterone, which promotes more visceral fat accumulation, which raises aromatase activity further. It runs in one direction unless something breaks it.
A 2016 review put the prevalence of testosterone deficiency in men with metabolic syndrome or type 2 diabetes at up to 50% — and identified waist circumference as the single strongest predictor of hypogonadism in this group (Ebrahimi & Christ-Crain, 2016). Testosterone deficiency and abdominal obesity don't just coexist. They sustain each other.
89.0% relative scale
higher hazard of type 2 diabetes in men aged 41-50 with low testosterone vs. normal T — propensity-matched cohort of 3.49 million men (Saffati et al., 2026)
How Common Is This Problem?
It's more common than most men realize, and it gets more common with age.
Among men in their 40s, biochemically confirmed low testosterone affects roughly 6-12% of the population (Canal de Velasco et al., 2025). But among men who already have obesity, metabolic syndrome, or type 2 diabetes, that prevalence climbs sharply — up to half of men in those groups have measurable testosterone deficiency.
A 2026 propensity-matched cohort study with more than 3.49 million participants found that men aged 41-50 with low testosterone had an 89% higher hazard of type 2 diabetes (HR 1.89) and a 44% higher hazard of metabolic syndrome (HR 1.44) compared to men with normal testosterone levels (Saffati et al., 2026). The associations were strongest in that 41-50 age window — which is exactly when many men first notice unexplained weight gain and write it off as "just getting older."
The relationship with body fat goes deeper than the scale. Testosterone deficiency was specifically associated with an HR of 1.49 for obesity in younger men (ages 18-30) — suggesting the hormonal disruption precedes, and may drive, the weight gain rather than simply accompanying it (Saffati et al., 2026).
Is It Low Testosterone or Just Getting Older?
Age-related testosterone decline is normal — roughly 1-2% per year after 30 — but biochemically confirmed hypogonadism is a diagnosable medical condition, not an inevitable part of aging. The clinical threshold is two total testosterone readings below 300 ng/dL on morning blood draws, combined with symptoms (Livingston et al., 2017). Those are different things, and conflating them leads men either to dismiss a real problem or to seek treatment they don't need.
The symptoms that prompt men to get tested — fatigue, reduced libido, difficulty building muscle, increased body fat, mood changes — overlap significantly with symptoms of other conditions. Symptoms alone don't establish the diagnosis.
Symptoms alone aren't enough. Plenty of men feel tired and gain weight for reasons that have nothing to do with testosterone — poor sleep, thyroid dysfunction, insulin resistance, caloric excess. Getting labs done is the only way to know which you're dealing with.
Two frequently missed drivers of low T that deserve mention: sleep deprivation and sleep apnea. One week of sleep restriction drops testosterone by approximately 15% in healthy young men. Sleep apnea suppresses nocturnal testosterone pulses and is extremely common in men with abdominal obesity — yet it often goes undiagnosed. Treating the sleep apnea doesn't always fully normalize testosterone, but it's a necessary first step.
For more on what to look for before going straight to labs, see low testosterone symptoms in men.
Fix the Cause First — Why Weight Loss Raises Testosterone
A meaningful number of men who come in asking about TRT don't end up needing it — because the real driver of their low testosterone is obesity, and the fix is upstream of the hormone.
In men with obesity-driven low testosterone — what clinicians call functional or secondary hypogonadism — the suppression is coming from the aromatase-excess loop described above. The HPG axis is intact and capable of producing normal testosterone. It's just being suppressed by elevated estradiol from visceral fat conversion.
For these men, meaningful weight loss can restore testosterone to normal without any medication. This has been shown consistently in bariatric surgery studies, dietary intervention trials, and increasingly with GLP-1 medications.
Semaglutide and tirzepatide — the GLP-1 receptor agonists used for weight loss — appear to raise testosterone indirectly by reducing visceral fat. One 2025 study found that semaglutide improved testosterone levels in obese men with functional hypogonadism (Gregorič et al., 2025). The mechanism is the aromatase pathway in reverse: less visceral fat means less aromatase activity, less T-to-estradiol conversion, and higher free testosterone.
This matters clinically because it reframes the question. If your low testosterone is being driven by obesity, the correct first-line intervention may be weight loss — not TRT. Your testosterone may normalize on its own once the visceral fat is addressed. If it doesn't, or if your testosterone is low for reasons other than obesity, that's when TRT becomes appropriate.
For more on how GLP-1 medications fit into this picture, see how GLP-1 medications work for weight loss.
TRT vs. Control: Metabolic Outcomes
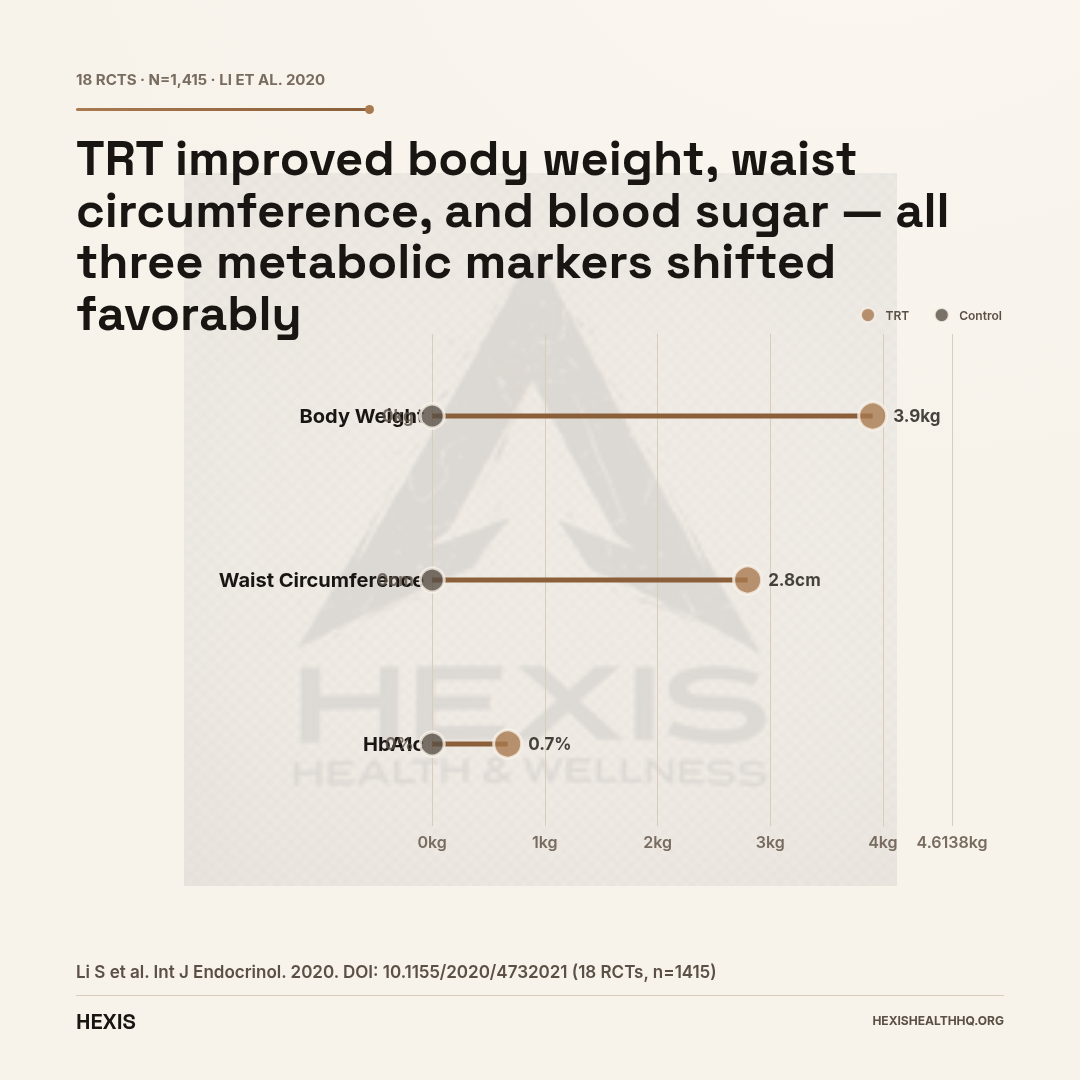
Meta-analysis of 18 RCTs in men with type 2 diabetes or metabolic syndrome (n=1,415) — Li et al., 2020
| Outcome | TRT Group | Control Group |
|---|---|---|
| Body weight change | −3.91 kg | No significant change |
| Waist circumference | −2.8 cm | No significant change |
| HbA1c | −0.67% | No significant change |
Source: Li S et al. Int J Endocrinol. 2020. DOI: 10.1155/2020/4732021
What TRT Actually Does to Body Composition
Testosterone replacement therapy produces body recomposition — less fat, more lean mass — not simple weight loss. In a meta-analysis of 18 randomized controlled trials (n=1,415), TRT reduced body weight by 3.91 kg, waist circumference by 2.8 cm, and HbA1c by 0.67% compared to control in men with type 2 diabetes or metabolic syndrome (Li et al., 2020). The scale may not shift dramatically, but body composition does.
Those numbers may look modest individually — but across a high-risk metabolic population (men already carrying T2DM or metabolic syndrome), they represent meaningful clinical improvements. The waist circumference reduction is particularly notable: waist tracks visceral fat specifically, which is the metabolically dangerous kind and the same fat that drives testosterone lower through aromatase conversion.
A 2024 systematic review focused on metabolic syndrome found that TRT produced statistically significant reductions in waist circumference (p=0.011) and triglycerides (p=0.039) in treated men (Mlynarz et al., 2024).
The European Menopause and Andropause Society (EMAS) position statement — based on review of available trial data — recommends considering TRT in hypogonadal men with insulin resistance or pre-diabetes, citing body composition improvements as one of the established benefits (Kanakis et al., 2023).
TRT Alone vs. TRT + Exercise: Why the Combination Matters
Here's a finding that changes how you should think about starting TRT: in a 2026 randomized controlled trial of 214 hypogonadal men followed for one year, TRT alone did not produce significant improvements in lean body mass or body fat percentage. Neither did exercise alone. Only the group combining TRT with structured exercise showed significant improvements in both lean mass and fat percentage at 6 and 12 months (Shigehara et al., 2026).
This is consistent with what the mechanism predicts. Testosterone creates the anabolic environment — it sensitizes muscle to training signals and reduces fat accumulation. But the signal that drives actual muscle protein synthesis is mechanical load. Without exercise, there's nothing for the testosterone to amplify.
If you're starting TRT expecting body recomposition to happen passively, the data says it probably won't. TRT + resistance training is what the evidence supports. One without the other is a partial solution.
A parallel finding from a 2025 trial: TRT combined with lifestyle therapy improved skeletal muscle glycolytic pathways in older obese hypogonadal men — suggesting TRT with lifestyle change produces metabolic adaptations at the tissue level that TRT alone does not (Viola et al., 2025).
If you want to understand what a full TRT protocol looks like and what to expect at each stage, how to treat low testosterone breaks it down in detail.
TRT and Heart Risk: What TRAVERSE Actually Found
TRAVERSE found TRT non-inferior to placebo for major adverse cardiovascular events and showed no increased risk of prostate cancer in treated men. A parallel analysis found TRT was associated with a 12% lower hazard of developing type 2 diabetes compared to controls (HR 0.88).
TRT requires monitoring: hematocrit, PSA, and testosterone levels at baseline and at least annually. TRT suppresses spermatogenesis — discuss fertility plans before starting.
Source: Bhasin S et al. JAMA Netw Open. 2023. PMID: 38150256
Is TRT Safe? The Cardiovascular Question Answered
TRT is not associated with increased cardiovascular risk in hypogonadal men — the TRAVERSE trial (n=5,246), the largest randomized safety trial to date, found TRT non-inferior to placebo for major adverse cardiovascular events and showed no increased prostate cancer risk (Bhasin et al., 2023). That finding settled a decade of uncertainty stemming from a 2010 study that raised concern about cardiovascular events in older men with mobility limitations.
TRAVERSE enrolled men with confirmed hypogonadism and elevated cardiovascular risk — exactly the population where concern was highest. The fact that even this high-risk group showed no signal is the relevant reassurance for most men considering TRT.
A secondary analysis found TRT significantly improved depressive symptoms compared to placebo in men with hypogonadism (Bhasin et al., 2024).
For the sexual function sub-trial (n=1,161), TRT improved sexual activity by an average of 0.49 acts per day compared to placebo at both 6 and 12 months — a finding notable for its persistence over the one-year follow-up (Pencina et al., 2024).
The 2026 large cohort study adds another data point: men on TRT had a hazard ratio of 0.88 for developing type 2 diabetes compared to hypogonadal men not on TRT — a statistically significant protective effect (Saffati et al., 2026).
One safety note that belongs in every TRT discussion: TRT suppresses spermatogenesis. If you want children, this must be discussed with your provider before starting. Alternatives like clomiphene or HCG exist for men who need to preserve fertility (Anaissie et al., 2017).
Monitoring requirements on TRT include hematocrit (TRT raises red blood cell production), PSA, and testosterone levels — at least at baseline and annually. The guidelines from the European Academy of Andrology (EAA) provide the standard monitoring framework (Corona et al., 2020).
Frequently Asked Questions
Does low testosterone cause belly fat specifically?
Yes. Low testosterone is most strongly linked to visceral fat — the fat stored around the abdominal organs — rather than subcutaneous fat. Visceral fat is also the type that drives metabolic risk. The connection is partly mechanical: visceral fat contains aromatase enzymes that convert testosterone to estradiol, which suppresses testosterone further. Men with larger waist circumferences tend to have lower testosterone levels, and the relationship strengthens with metabolic syndrome (Ebrahimi & Christ-Crain, 2016).
Will TRT make me lose weight?
TRT is not a weight-loss drug. In trials, men on TRT see modest reductions in body weight — averaging 3.91 kg in one large meta-analysis (Li et al., 2020) — but the more meaningful change is the shift in body composition: less fat, more lean mass. The scale may not move much. Your body shape, strength, and metabolic profile can change significantly, especially when TRT is combined with resistance training (Shigehara et al., 2026).
Can losing weight raise my testosterone levels?
Yes — and for men whose low testosterone is driven by obesity, weight loss may restore testosterone to normal without TRT. The mechanism is the aromatase pathway: reducing visceral fat lowers aromatase activity, reduces testosterone-to-estradiol conversion, and allows the HPG axis to restore testosterone production. GLP-1 medications that produce significant visceral fat loss appear to raise testosterone through this same mechanism (Gregorič et al., 2025).
How long does TRT take to affect body composition?
Meaningful changes in body composition typically emerge at 3-6 months. In the RCT by Shigehara et al. (2026), significant differences between the TRT+exercise group and controls were visible at the 6-month measurement point and maintained through 12 months. Fat reduction tends to be more visible earlier than lean mass gains. Setting realistic expectations matters — TRT is not a rapid transformation.
Do I need TRT, or should I lose weight first?
That depends on what's driving your low testosterone. If obesity is the primary cause — meaning your HPG axis is suppressed by excess visceral fat and high aromatase activity — weight loss may normalize your testosterone without medication. If your testosterone is low for reasons unrelated to obesity (primary hypogonadism, pituitary dysfunction, prior injury), TRT is appropriate regardless of weight. Diagnosis requires labs, not guesswork. Two morning testosterone draws below 300 ng/dL with symptoms is the clinical threshold (Livingston et al., 2017).
The Bottom Line
Low T promotes visceral fat accumulation and loss of lean mass. Visceral fat drives testosterone lower through aromatase-mediated conversion. Once that cycle starts, it tends to persist — and standard advice to "just eat better and exercise" doesn't address the hormonal side of it.
If your testosterone is biochemically low, TRT can improve body composition. The evidence is clear: modest but real reductions in body weight, measurable decreases in waist circumference, and improved metabolic markers in men with type 2 diabetes and metabolic syndrome. The combination of TRT with structured exercise produces significantly better outcomes than either alone.
TRT is not a shortcut, and it's not for everyone. But for men with confirmed hypogonadism who've been watching their waistline expand despite real effort, it's a medically appropriate intervention backed by strong trial data.
If you want to find out whether low testosterone is contributing to your weight changes, it starts with the right labs — not with a guess.
Schedule a consultation and your HEXIS provider will review your full hormone panel before recommending anything.
Does Low Testosterone Cause Weight Gain? The Bottom Line
- 1
Low testosterone and visceral fat drive each other in a self-reinforcing loop — aromatase in fat tissue converts testosterone to estradiol, suppressing production further. Up to 50% of men with metabolic syndrome or type 2 diabetes have measurable testosterone deficiency.
- 2
TRT produces body recomposition, not simple weight loss — average 3.91 kg body weight reduction and 2.8 cm waist reduction in a meta-analysis of 18 RCTs. The combination of TRT with exercise produces significantly better results than either alone.
- 3
If obesity is driving your low testosterone, weight loss alone may restore normal T without medication. Get labs before assuming you need TRT — two morning draws below 300 ng/dL with symptoms is the clinical threshold.