Enclomiphene: Benefits, Dosing & Evidence
Enclomiphene: Benefits, Dosing & Evidence
Most testosterone treatments work by replacing your body's production. Enclomiphene does something different — it convinces your own system to produce more. If you're a man with low testosterone who still wants to have children, that difference matters more than almost anything else your doctor could tell you.
The short answer: Enclomiphene citrate is a SERM (selective estrogen receptor modulator) that blocks hypothalamic estrogen receptors, prompting the body to release more LH and FSH and drive testosterone production from within. Phase II and III trials showed it normalizes testosterone while preserving sperm counts — unlike testosterone gel, which suppresses both LH/FSH and fertility. It is not FDA-approved; legal US access requires a physician prescription through a compounding pharmacy.
What Is Enclomiphene and How Does It Work?
Standard testosterone replacement therapy has one fundamental problem: it shuts down your own hormone signal. When you apply testosterone gel or inject testosterone, your hypothalamus reads those rising levels and stops releasing the hormones that tell your testes to work. LH goes down. FSH goes down. Sperm production drops — sometimes to zero.
Enclomiphene works upstream. It blocks estrogen receptors at the hypothalamus, which makes the brain think estrogen is too low and doubles down on releasing LH and FSH. Those signals reach the testes and drive testosterone production from within. The factory stays open.
Clomiphene citrate (generic Clomid) has been used off-label for this purpose in men for decades. But clomiphene is a 50/50 mixture of two isomers: enclomiphene (the trans-isomer) and zuclomiphene (the cis-isomer). The testosterone-raising effect comes primarily from enclomiphene (Ghobadi et al., 2009), while zuclomiphene accumulates in the body — its half-life is measured in weeks rather than hours — and it's responsible for the visual disturbances and mood effects clomiphene users sometimes report (Ghobadi et al., 2009).
Enclomiphene citrate removes zuclomiphene from the equation entirely. What you're left with is the mechanistically active isomer, without its problematic partner. For context on how SERMs and other agents compare to direct testosterone therapy, see our breakdown of low testosterone symptoms and treatment options.
Tier 1 controlled trials with enclomiphene as the study compound — Phase II and Phase III RCTs with verified DOIs
What Does the Clinical Evidence Actually Show?
Enclomiphene has more Phase II and Phase III trial data behind it than most compounds discussed in the testosterone-optimization space.
Phase II: Testosterone Up, Sperm Preserved
The ZA-203 Phase II randomized controlled trial (Wiehle et al., 2014) compared enclomiphene citrate directly against topical testosterone in men with secondary hypogonadism. The result was the clearest possible illustration of the fertility problem with standard TRT.
Both treatments raised testosterone to normal range. The key difference: in the testosterone gel group, sperm counts dropped. In the enclomiphene group, sperm counts were maintained — and LH and FSH both increased, confirming the upstream mechanism was working as intended (Wiehle et al., 2014).
This is not a subtle finding. It's the central clinical case for enclomiphene: you can restore testosterone without dismantling fertility.
Phase III: The Obese Hypogonadal Men Trials (ZA-304 and ZA-305)
Kim, McCullough, and Kaminetsky (2016) published results from two parallel Phase III trials comparing enclomiphene (12.5 mg and 25 mg daily) against testosterone gel 1.62% in overweight men with secondary hypogonadism — defined as morning testosterone at or below 300 ng/dL over 16 weeks.
Again, both treatments brought testosterone into range. Again, the testosterone gel arm saw LH and FSH suppressed and sperm concentration fall. In the enclomiphene arm, LH and FSH rose, and sperm concentration was preserved (Kim et al., 2016).
The Phase III data is where the regulatory story also becomes relevant: Repros Therapeutics, the original developer, filed NDA 022201 for Androxal (their branded enclomiphene product). The FDA issued a Complete Response Letter in 2013, declining approval. The rejection was not primarily a safety ruling — it was a regulatory data package issue. The drug never reached market.
Phase III: Comparison to Testosterone Gel (ZA-301)
Kaminetsky, Werner, Fontenot, and Wiehle (2013) published an earlier Phase III trial directly comparing enclomiphene citrate to testosterone gel in men with low testosterone. The findings reinforced the same pattern: enclomiphene stimulated endogenous testosterone production while the gel route suppressed the body's own signaling (Kaminetsky et al., 2013).
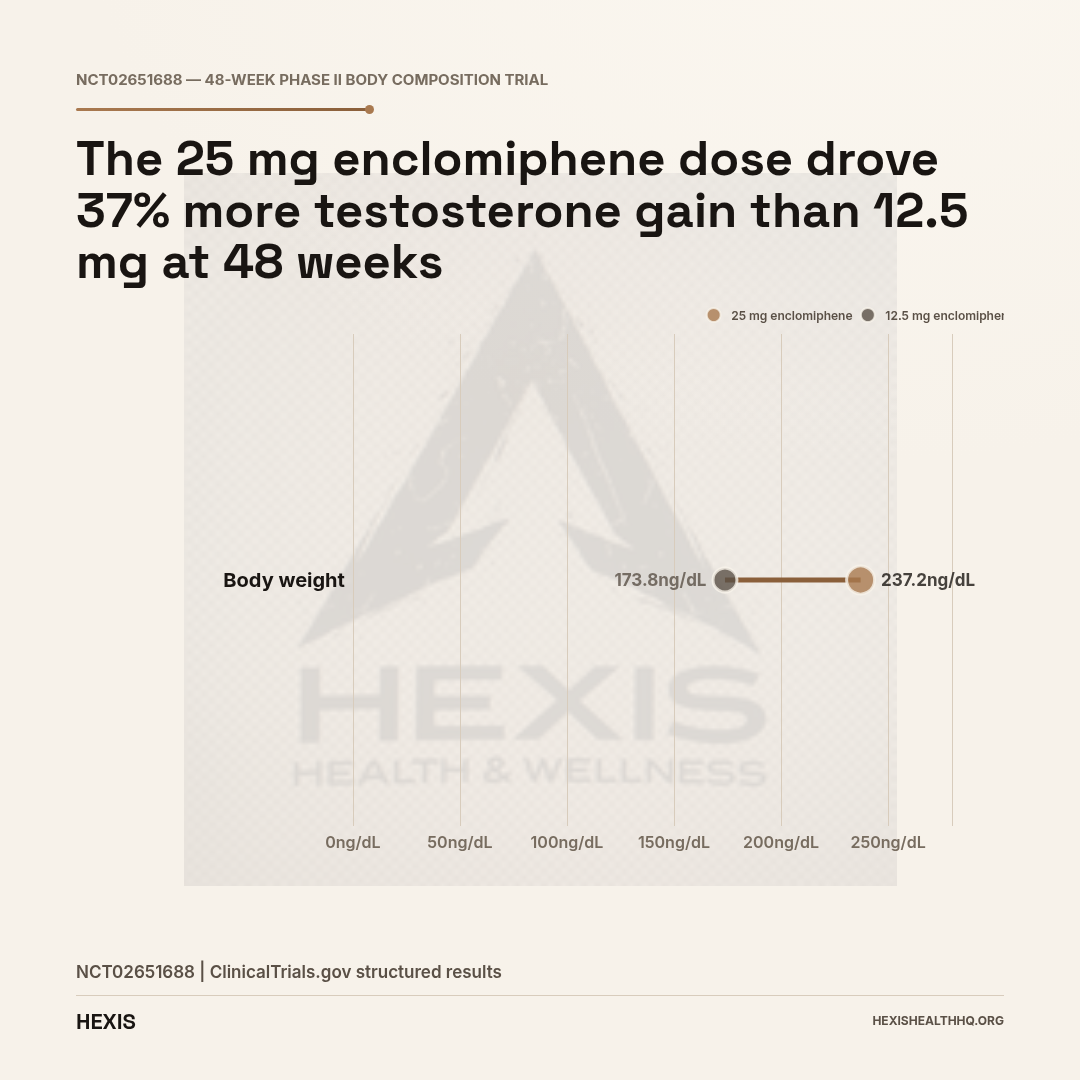
Body Composition at 48 Weeks (NCT02651688)
A completed Phase II multicenter study (NCT02651688) tracked men with acquired hypogonadotropic hypogonadism on 12.5 mg or 25 mg enclomiphene plus diet and exercise over 48 weeks. Baseline LH levels were approximately 3.41–3.93 mIU/mL. Lean body mass at baseline ran approximately 65–68 kg across groups. By week 48, participants on enclomiphene gained lean mass — up to 3.14 kg in one arm — alongside improvements in body strength on both chest press and leg press metrics (NCT02651688).
Is Enclomiphene Better Than Clomid for Men?
For men with secondary hypogonadism, enclomiphene is generally the preferred SERM over generic clomiphene — primarily because it does not contain zuclomiphene, the cis-isomer responsible for side effects including vision disturbances and mood changes. Both raise testosterone via the same hypothalamic mechanism; enclomiphene does it without the pharmacokinetic liability of zuclomiphene accumulation.
Clomiphene (Clomid) raises testosterone in men via the same mechanism: it blocks hypothalamic estrogen receptors. Multiple studies and decades of off-label use confirm it works. The problem is the zuclomiphene load.
Zuclomiphene has a half-life of approximately 30 days, compared to enclomiphene's shorter elimination (Ghobadi et al., 2009; Ghobadi et al., 2009). With daily clomiphene dosing, zuclomiphene accumulates. That accumulation is associated with the mood instability and visual disturbances that make some men stop clomiphene treatment.
Enclomiphene eliminates that accumulation because it contains no zuclomiphene. Whether that translates into meaningfully fewer side effects in clinical practice is harder to establish given that head-to-head trial data comparing long-term tolerance of enclomiphene versus clomiphene in men is limited. But the pharmacokinetic rationale is real (Ghobadi et al., 2009).
The HPT axis research by Miller and colleagues (Miller et al., 2019) examined the hypothalamic-pituitary-testicular axis effects following clomiphene administration in males — including urinary detection windows relevant to anti-doping surveillance. That work highlights how both isomers are detectable and how the axis responds to SERMs more broadly.
Enclomiphene vs. Testosterone Replacement Therapy
Key differences across Phase II/III trials — Wiehle 2014, Kim 2016, Kaminetsky 2013
| Enclomiphene | Testosterone Gel / Injections | |
|---|---|---|
| Raises testosterone to normal range | Yes | Yes |
| LH & FSH after treatment | Increases | Suppresses |
| Sperm production | Preserved | Reduced or eliminated |
| Mechanism | Stimulates endogenous production | External replacement |
| FDA-approved | No | Yes |
| Long-term safety data | Limited (16 wk trials) | Extensive |
| Access pathway | Compounding Rx only | Standard pharmacy Rx |
| WADA status | Prohibited at all times | Not prohibited (TUE available) |
Source: Wiehle et al. (Fertil Steril, 2014); Kim et al. (BJU Int, 2016); Kaminetsky et al. (J Sex Med, 2013)
Enclomiphene vs. Testosterone Replacement Therapy: The Core Trade-Off
The core difference between enclomiphene and testosterone replacement therapy is this: TRT raises testosterone by supplying it externally and shutting down the body's own production signal; enclomiphene raises testosterone by amplifying the body's own signal while leaving production intact. That distinction determines everything else — including fertility outcomes.
Testosterone gel or injections will raise your testosterone. In most cases, they'll raise it reliably, predictably, and with a well-understood side effect profile. TRT also has strong long-term cardiovascular safety data. What it will not do is preserve your fertility. It suppresses LH and FSH. It reduces — sometimes eliminates — sperm production. If you're on TRT and you want to have children, you need to be doing something else alongside it.
Enclomiphene preserves fertility. That is its primary clinical use case. Every Phase II and Phase III trial showed this. LH and FSH go up, not down. Spermatogenesis continues (Wiehle et al., 2014; Kim et al., 2016; Kaminetsky et al., 2013).
The trade-off is certainty and approval. TRT is FDA-approved, has decades of prescribing history, and has standard dosing protocols. Enclomiphene is not FDA-approved, has no manufacturer, and is available only through 503A compounding pharmacies. Clinical trial data is solid through 16 weeks for testosterone and sperm outcomes; long-term safety data beyond that window is limited.
If fertility is not a concern, standard TRT is generally the cleaner clinical pathway. If you want to raise testosterone without shutting down your reproductive axis — and you have secondary hypogonadism — enclomiphene is worth a serious conversation with a physician. For men who want to understand the full picture of available testosterone-restoration options, our testosterone booster guide covers the evidence spectrum from lifestyle interventions to pharmaceutical approaches.
Who Is — and Isn't — a Candidate?
Enclomiphene only works if the problem is upstream. Specifically, it works in secondary hypogonadism, where the testes are functional but the hypothalamic-pituitary signal is insufficient. When we evaluate patients for enclomiphene at HEXIS, the first question is always: is the LH low or is the testosterone low because the testes can't respond? The answer to that question determines whether enclomiphene has anything to work with.
If you have primary hypogonadism — where the testes themselves are the problem (Klinefelter syndrome, testicular injury, chemotherapy damage) — enclomiphene has nothing to work with. You can flood the axis with LH and FSH signals and the testes still won't produce testosterone if they're not capable of doing so. Enclomiphene is not effective for primary hypogonadism.
Who should NOT use enclomiphene: Men with primary hypogonadism (high LH, low testosterone); athletes subject to WADA/USADA anti-doping testing (prohibited at all times, S4.3); anyone seeking a prescription-free or online-without-physician route (no legal pathway exists); men with a history of thromboembolic events (SERMs carry a class-level risk that should be discussed with a physician before starting).
Secondary hypogonadism — also called hypogonadotropic hypogonadism — is the target population for every enclomiphene trial (Rodriguez et al., 2016). It's also the most common form of low testosterone in overweight and middle-aged men, where central signaling issues, insulin resistance, and sleep dysfunction all contribute to suppressed LH and FSH. If you're unsure which type applies to you, read our article on low testosterone symptoms — it covers how to interpret your LH and FSH results alongside total testosterone.
A 2020 review by Achua, Frech, and Ramasamy examined stem cell and emerging therapies for hypogonadism, contextualizing where SERM-based approaches fit among future treatment options (Achua et al., 2020).
The 2025 review by Hochu, Geyer-Kim, and Kim in Translational Andrology and Urology examined how to preserve spermatogenesis in testosterone deficiency, covering both replacement and stimulatory approaches — and identified enclomiphene as the leading oral agent in the stimulatory category (Hochu et al., 2025).
daily — the only dose range studied in Phase II and Phase III controlled trials. No FDA-approved prescribing information exists.
What Dose Is Used, and What Does the Evidence Support?
The Phase II and Phase III trials used 12.5 mg and 25 mg daily. Those are the only doses with controlled trial data (Wiehle et al., 2014; Kim et al., 2016; Kaminetsky et al., 2013).
The 25 mg dose generally produced stronger testosterone responses. The 12.5 mg dose was better tolerated by some participants.
There is no FDA-approved prescribing information because there is no FDA-approved product. Physicians prescribing enclomiphene through compounding pharmacies are operating outside standard dosing guidelines, relying on the trial literature to inform dosing decisions. 6.25 mg starting doses are used clinically but have no formal trial support. Split-week dosing (e.g., three times per week) is discussed in clinical communities but similarly lacks Phase III data.
12.5 mg to 25 mg daily is what the trials studied. That's the range with evidence. Everything else is extrapolation. In clinical practice at HEXIS, we treat the 12.5 mg dose as the starting point — it's where the Phase III trials established efficacy with the best tolerability profile — and adjust based on labs at 4-6 weeks.
What Are the Side Effects?
The side effect data is limited by the relatively short duration of the Phase III trials (primarily 16 weeks). What was reported in trials and in clinical practice includes:
- Vision disturbances — occasionally reported, though less frequently than with generic clomiphene, consistent with the absence of zuclomiphene
- Mood changes — generally milder than clomiphene
- Acne — related to the rise in testosterone
- Elevated estrogen — testosterone aromatizes to estradiol; higher testosterone means more potential estrogen; some men need an aromatase inhibitor alongside enclomiphene
- Testicular discomfort — occasionally reported, transient
The FDA's FAERS database contains 10 adverse event reports on record for enclomiphene. That low number reflects the limited use through compounding channels rather than a clean safety profile — it means fewer people have used it, so there are fewer reports. It is not evidence of exceptional safety.
Long-term safety data beyond 16 weeks is genuinely thin. If you're considering enclomiphene long-term, that gap needs to be part of your conversation with a physician.
Not FDA-Approved — WADA-Prohibited for All Athletes
NDA 022201 (Androxal) received a Complete Response Letter from the FDA in 2013 and never reached market. Enclomiphene is also listed under WADA S4.3 — Hormone and Metabolic Modulators — prohibited at all times with no therapeutic use exemption pathway for athletes.
Legal US access requires a physician prescription filled at a 503A compounding pharmacy. Purchasing enclomiphene without a prescription or from research-chemical vendors is not a legal pathway.
Source: FDA NDA 022201; WADA Prohibited List S4.3; brief.regulatoryStatus
What Is Enclomiphene's Legal Status?
This is not a gray area, and it's worth being clear.
FDA status: Enclomiphene is not FDA-approved. NDA 022201 (Androxal) received a Complete Response Letter in 2013. The Androxal brand never reached market. There is no FDA-approved version of enclomiphene available in the United States as of 2026.
How people legally access it: Through 503A compounding pharmacies with a physician prescription. Physicians can prescribe enclomiphene off-label, and compounding pharmacies can produce it. This is the legal pathway. Purchasing enclomiphene without a prescription, from research-chemical vendors, or via overseas sources is not a legal pathway.
WADA status: Enclomiphene is prohibited at all times under WADA S4.3 — Hormone and Metabolic Modulators (SERMs). Any athlete subject to WADA or USADA testing who uses enclomiphene — for any reason, with any prescription — is at risk of a positive test. There is no therapeutic use exemption pathway that changes this. Athletes cannot use enclomiphene.
International status: Enclomiphene is not approved in the UK (not MHRA authorized), Australia (not on the ARTG), Canada (not listed in Health Canada's Drug Product Database), or by the EMA in the European Union. Access internationally follows similar compounding or off-label pathways where local law permits.
Ongoing Research
Enclomiphene has an active clinical trial record despite its FDA rejection in 2013. At least four completed Phase II/III trials registered on ClinicalTrials.gov examined testosterone normalization, body composition, and bone mineral density outcomes across several hundred participants — and research continues. Active and recently completed trials include:
- NCT01739595 — Phase III study evaluating morning testosterone normalization in overweight men with secondary hypogonadism (181 participants, completed, results available)
- NCT02651688 — Phase II body composition study at 48 weeks with 12.5 mg and 25 mg doses (completed, results available)
- NCT01739582 — Extension study of enclomiphene citrate in secondary hypogonadism treatment (300 participants, Phase III, completed)
- NCT01619683 — Phase III assessment of enclomiphene's effects on bone mineral density in secondary hypogonadism (300 participants)
The Rodriguez, Pastuszak, and Lipshultz (2016) review in Expert Opinion on Pharmacotherapy summarized the clinical development timeline and regulatory history, making it the most useful single source on where enclomiphene sits as an investigational agent (Rodriguez et al., 2016).
Frequently Asked Questions
What is enclomiphene and how is it different from Clomid?
Enclomiphene is the trans-isomer of clomiphene. Clomid (generic clomiphene) is a 50/50 mix of two isomers: enclomiphene and zuclomiphene. The testosterone-raising effect comes primarily from enclomiphene. Zuclomiphene has a long half-life and accumulates with daily dosing — it's linked to the visual and mood side effects some men report on Clomid. Enclomiphene contains no zuclomiphene.
Can I use enclomiphene instead of TRT to keep my fertility?
If you have secondary hypogonadism, yes — this is exactly what enclomiphene was developed for. Phase II and III trials showed it raised testosterone to normal range while LH, FSH, and sperm counts all stayed intact or improved. Testosterone gel and injections do the opposite: they raise testosterone while suppressing LH, FSH, and sperm production. If preserving fertility is a priority, enclomiphene is the clinically supported alternative worth discussing with your physician.
How long does enclomiphene take to work?
Testosterone response was measurable within weeks in Phase III trials. Most protocols check labs at 4-6 weeks to assess response. The 16-week trial duration was chosen because it's long enough to see sustained hormonal changes. How quickly you personally respond depends on your baseline LH/FSH levels, body composition, and whether secondary hypogonadism is the correct diagnosis.
Does enclomiphene cause vision side effects like clomiphene?
Vision disturbances are occasionally reported with enclomiphene, but the pharmacokinetic rationale is that they should be less common than with generic clomiphene — because zuclomiphene, which accumulates with daily dosing, is absent. Clinical reports are consistent with that. Vision issues are not eliminated, but they appear less frequent. If you experience visual changes on enclomiphene, stop and contact your prescribing physician.
Does enclomiphene increase estrogen?
It can. Enclomiphene raises testosterone, and testosterone aromatizes into estradiol. Higher testosterone generally means higher estrogen, especially in men with higher body fat (adipose tissue contains aromatase). Some men on enclomiphene need an aromatase inhibitor to manage estrogen levels. This is why regular lab monitoring — not just testosterone, but full hormone panels — matters when using enclomiphene off-label.
Working With a Physician on Enclomiphene
Because enclomiphene is off-label and compounded, the quality of prescribing varies significantly between providers. What the clinical evidence supports — and what reasonable clinical practice looks like — includes:
- Confirming secondary hypogonadism before prescribing. Lab work needs to show low testosterone alongside low-normal or low LH and FSH. High LH with low testosterone suggests primary hypogonadism — enclomiphene won't help.
- Starting at 12.5 mg, the lower Phase III trial dose, and adjusting based on labs at 4-6 weeks.
- Monitoring estradiol, not just testosterone. Enclomiphene can drive estrogen up alongside testosterone.
- Setting realistic time horizons. Fertility outcomes and testosterone normalization take weeks. The 16-week trial window exists for a reason.
- Having an honest conversation about long-term data. There isn't much beyond 16 weeks. That's not a reason to avoid it if the indication fits — it's a reason to monitor carefully and reassess.
At HEXIS, we start with labs — not guesswork. If enclomiphene is worth considering in your case, that conversation happens after we understand your full hormone panel, not before. Schedule a consultation to get your labs ordered and reviewed by a physician who understands this space.
Enclomiphene: The Bottom Line
- 1
Enclomiphene raises testosterone by working upstream — it stimulates your own LH and FSH rather than replacing testosterone externally. Multiple Phase II and III trials confirm it raises T to normal range while preserving sperm production, which no form of TRT does.
- 2
It is not FDA-approved and carries a WADA prohibition at all times. The only legal US pathway is a physician prescription through a 503A compounding pharmacy. Athletes subject to anti-doping testing cannot use it. Long-term safety data beyond 16 weeks is limited.
- 3
The right candidate is a man with confirmed secondary hypogonadism — low T alongside low-normal LH and FSH — who wants to restore testosterone without shutting down fertility. Primary hypogonadism does not respond to enclomiphene. Start with labs, not assumptions.