Jatenzo: Oral Testosterone Explained — How It Works, Dosing, and What the Data Show
Jatenzo Oral Testosterone Explained — How It Works, Dosing, and What the Data Show
Most men on testosterone replacement therapy have dealt with weekly injections, daily gel applications that require gloves and careful skin coverage, or tiny pellets inserted under the skin. Jatenzo oral testosterone changed that equation in 2019 — it is a twice-daily capsule you take with food. No needles, no transfer risk, no clinic visits for administration.
But Jatenzo is not just a more convenient form of the same old approach. It solves a specific pharmacology problem that kept oral testosterone off the US market for decades. Here is what the science actually shows about how it works, how well it works, and what you need to know about the risks before considering it.
The short answer: Jatenzo is an FDA-approved oral testosterone undecanoate capsule taken twice daily with a meal containing at least 19 grams of fat. In phase III trials, it restored testosterone to the normal range in 84–87% of hypogonadal men (Swerdloff et al., 2020). It carries a boxed warning for blood pressure increases — a real signal worth taking seriously — but it does not carry the liver toxicity concern associated with older oral androgens.
Why Was There No FDA-Approved Oral Testosterone Before 2019?
The liver is the reason oral testosterone had no US approval for so long. When you swallow most drugs, they pass through the portal vein into the liver before reaching systemic circulation — a process called hepatic first-pass metabolism. For testosterone, this is devastating. The liver breaks it down so aggressively that almost none reaches the bloodstream in active form. Older oral androgens like methyltestosterone got around this by adding a chemical modification at the 17-alpha position, which blocks liver metabolism — but that same modification causes liver toxicity, including peliosis hepatis and hepatocellular carcinoma (Patel et al., 2022).
Testosterone undecanoate takes a completely different route. As a long-chain fatty acid ester dissolved in castor oil and propylene glycol laurate, it is too lipophilic for portal absorption. Instead, it is packaged into chylomicrons — the fat-transport particles your gut uses after a fatty meal — and carried through the intestinal lymphatic system directly into the thoracic duct and then systemic circulation (Shackleford et al., 2003). The liver is bypassed almost entirely. Animal studies showed that between 91.5% and 99.7% of the systemically available testosterone undecanoate arrived via lymphatic transport rather than portal absorption (Shackleford et al., 2003). Because it bypasses the liver, there is no 17-alpha alkylation needed, and no hepatotoxicity observed in any phase III trial.
This lymphatic mechanism is what distinguishes Jatenzo from every previous attempt at oral testosterone replacement therapy — the drug reaches systemic circulation before the liver ever sees it.
This is why Jatenzo is structurally distinct from injectable testosterone undecanoate (Aveed). Aveed is a deep intramuscular injection given every 10 weeks in a clinical setting with a 30-minute post-injection observation period due to pulmonary oil microembolism risk. Jatenzo is an oral capsule. Same molecule, fundamentally different delivery system and risk profile.
How Does Food Affect Jatenzo Absorption?
Food is not optional with Jatenzo — it is the mechanism. Because testosterone undecanoate requires lymphatic transport triggered by fat absorption, eating too little fat with the capsule causes a dramatic drop in drug exposure.
A four-way crossover pharmacokinetic study quantified exactly how much this matters. With a near-fasting meal containing only 0.6 grams of fat, the testosterone AUC was 30.7 nmol·h/L. With a moderate meal containing 19 grams of fat, AUC jumped to 146 nmol·h/L. Increasing fat further to 44 grams produced no meaningful additional benefit — AUC was 154 nmol·h/L (Schnabel et al., 2007). You need at least 19 grams of fat per meal, but you don't need a high-fat meal. Two eggs and avocado toast, a handful of nuts with a protein shake, a normal lunch — all of those work.
The FDA label sets the minimum fat threshold at 19 grams per meal for both the morning and evening doses. Taking Jatenzo on an empty stomach or with a very low-fat meal could reduce drug exposure by roughly five-fold compared to a normal meal. That is not a pharmacist's footnote — it is the core requirement for the drug to work.
Jatenzo Dosing and Titration
Jatenzo is prescribed as twice-daily (BID) dosing, taken with both meals. The approved dose range runs from 158 mg to 396 mg per capsule, taken twice daily. The starting dose is 158 mg BID.
Dose adjustment happens in a specific, protocol-driven way. About four to six hours after the morning dose, your average testosterone concentration (Cavg) can be measured from a single blood draw. The prescriber uses that Cavg to titrate the dose at four-week intervals. The target is a Cavg in the eugonadal range of 300–1,000 ng/dL. Understanding what low testosterone symptoms feel like can help clarify whether that Cavg is actually translating into clinical improvement.
Peak concentration (Tmax) occurs approximately four to five hours after each dose. This pharmacokinetic pattern differs meaningfully from injections, which produce supraphysiological peaks in the days after injection and sub-physiological troughs by week two or three, and from gels, which provide more stable daily absorption but require consistent application and skin-to-skin transfer precautions.
“Over 24 months of uninterrupted oral testosterone undecanoate therapy, mean serum testosterone concentrations stayed in the eugonadal range — and sexual function scores improved significantly at every measured time point.”
What the Phase III Trials Actually Found
Jatenzo restored testosterone to the eugonadal range in 84–87% of hypogonadal men across two pivotal phase III randomized trials, with efficacy sustained through a two-year extension study — all trials specific to the Jatenzo formulation.
Trial II (PMID 32382745): 166 hypogonadal men were randomized 3:1 to oral testosterone undecanoate (Jatenzo) or Axiron topical testosterone for three to four months. The primary endpoint was achieving a eugonadal average testosterone concentration. Results: 87% of Jatenzo-treated men reached the eugonadal range, with a mean serum T Cavg of approximately 489 ng/dL. The topical testosterone arm achieved the same 87% rate. Mean systolic blood pressure increased 3 to 5 mmHg with Jatenzo (Swerdloff et al., 2020).
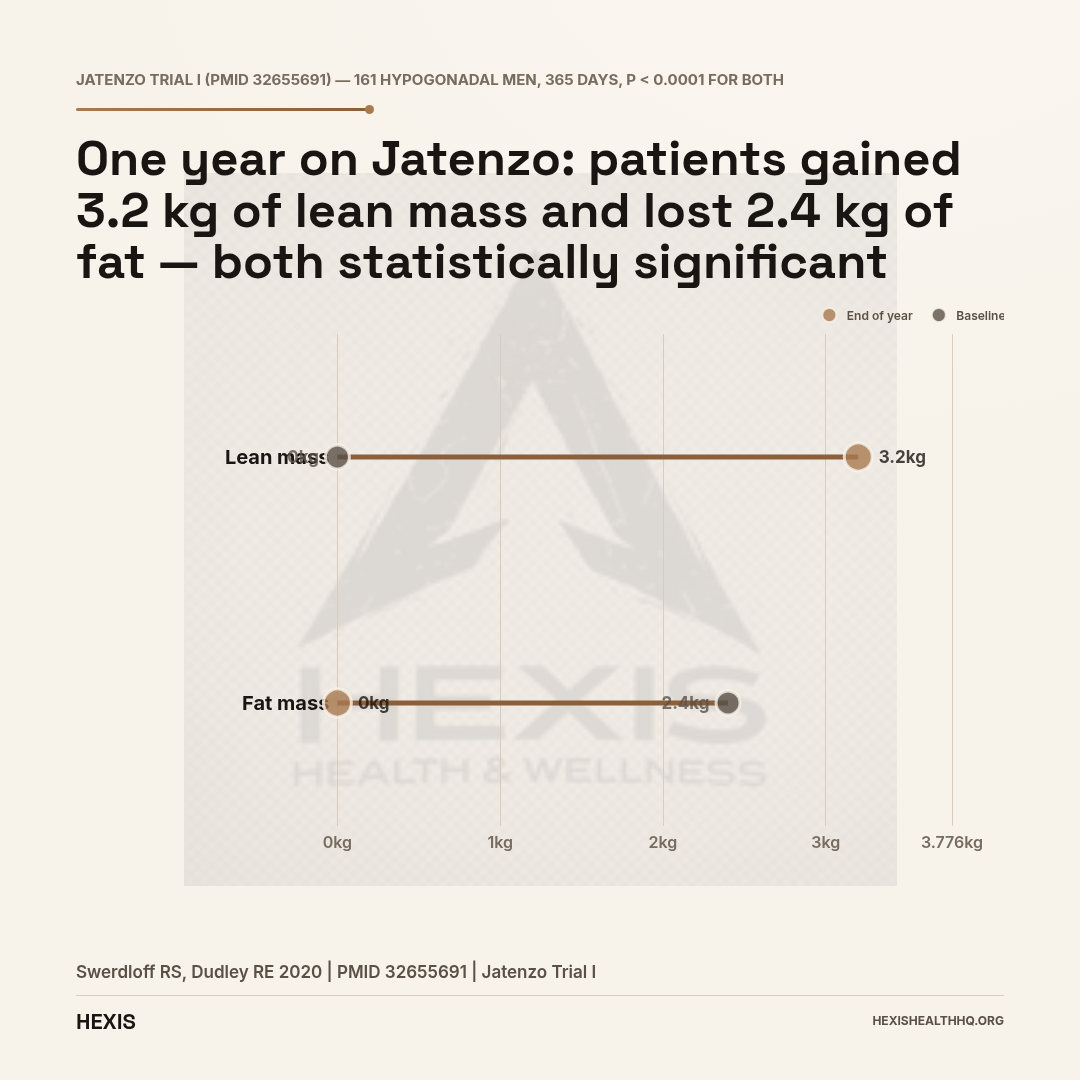
Trial I (PMID 32655691): 161 hypogonadal men received Jatenzo for 365 days versus 160 receiving testosterone gel. The eugonadal success rate was 84%, with a mean T Cavg of 628 ng/dL. Beyond testosterone levels, the year-long trial captured body composition data: lean mass increased by 3.2 kg and fat mass decreased by 2.4 kg, both reaching statistical significance (p < 0.0001). Bone density improved at both the hip (+0.012 g/cm²) and spine (+0.018 g/cm²) (Swerdloff & Dudley, 2020).
Two-year extension (PMID 36272969): Of 129 eligible Jatenzo-treated subjects from Trial I, 69 completed an additional 12 months, reaching 24 months of uninterrupted oral testosterone undecanoate therapy. Mean T Cavg remained in the eugonadal range at 617 ng/dL. Sexual function scores (Psychosexual Daily Questionnaire) improved significantly at all time points (p < 0.0011 for all domains). Hematocrit increased slightly but stayed below 48% throughout. Prostate-specific antigen changes were not clinically significant. HDL cholesterol decreased by 9.8 mg/dL from baseline (Honig et al., 2022).
These findings hold alongside the broader oral testosterone undecanoate literature. A six-month phase III single-arm trial of Kyzatrex in 155 hypogonadal men found 87.8% (worst-case) and 96.1% of completers achieved eugonadal plasma testosterone, with a mean serum T Cavg of 452 ng/dL (Bernstein & Dhingra, 2024). A 2025 phase III trial of Tlando in 315 men found 87.4% achieved eugonadal Cavg, with nominally significantly greater improvements in mental health scores compared to gel (Miner et al., 2025).
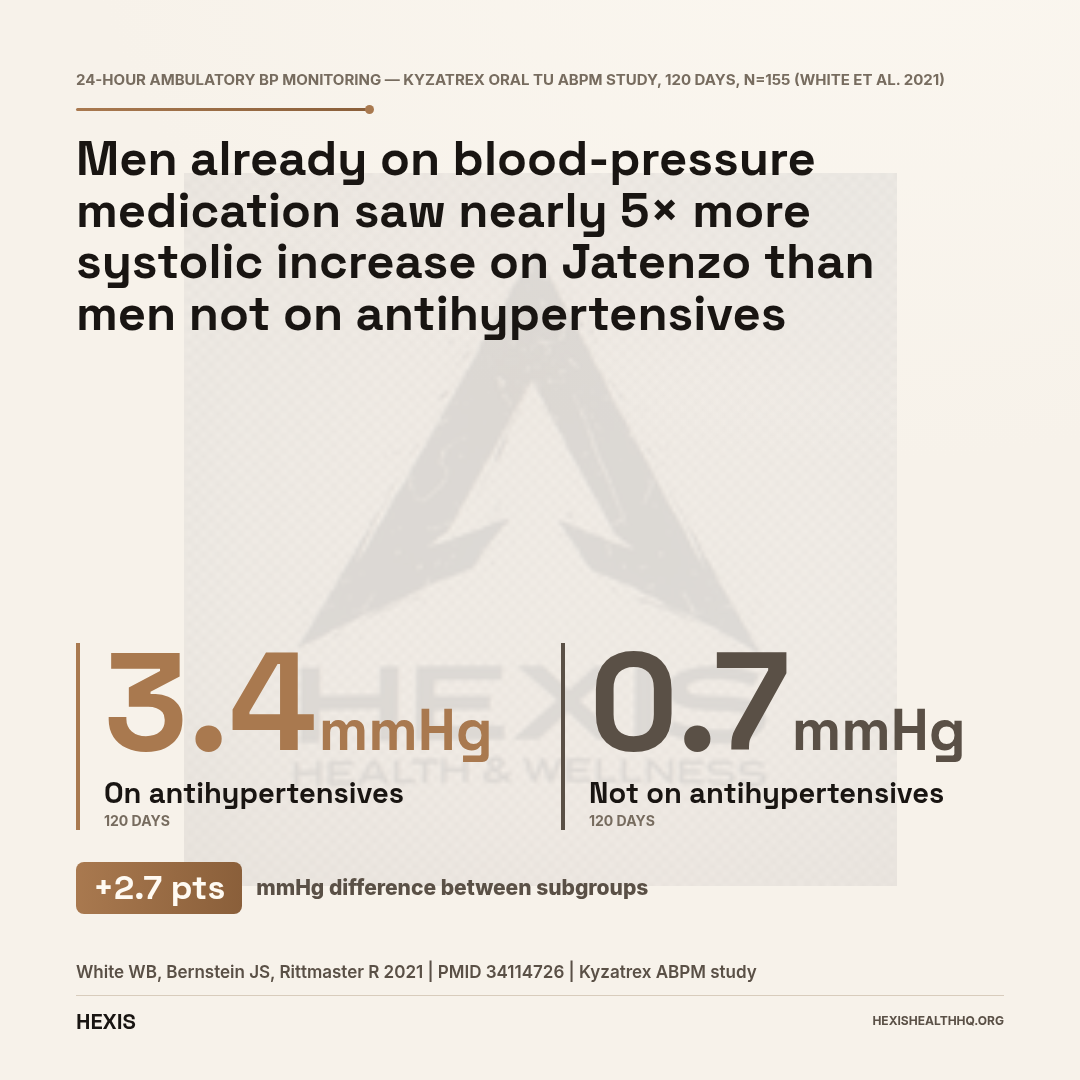
Jatenzo carries an FDA boxed warning for blood pressure increases that can raise the risk of major adverse cardiovascular events (MACE). In phase III trials, systolic BP increased 3–5 mmHg on average. Men on antihypertensive medication saw 3.4 mmHg increases vs 0.7 mmHg in non-medicated men. BP must be measured before starting, during, and after treatment. Jatenzo is contraindicated in men with uncontrolled hypertension.
Source: FDA prescribing information; White et al., 2021 — PMID 34114726
What Is the Boxed Warning About Blood Pressure?
Jatenzo carries an FDA boxed warning — the highest warning level the agency issues — for blood pressure increases that can raise the risk of major adverse cardiovascular events (MACE): non-fatal heart attack, non-fatal stroke, and cardiovascular death. This is not a theoretical concern buried in the label. It is the central safety monitoring requirement for every patient on this drug.
Across trials, systolic blood pressure increased 3 to 5 mmHg on average with Jatenzo (Swerdloff et al., 2020). In the two-year follow-up, the increase was in the range of 3 to 6 mmHg (Honig et al., 2022). Ambulatory blood pressure monitoring data from Kyzatrex — another oral testosterone undecanoate formulation — found a mean systolic increase of 1.7 mmHg overall (95% CI: 0.3–3.1 mmHg), but the effect was not uniform: men already taking antihypertensive medication saw a 3.4 mmHg increase, while men not on antihypertensives saw only a 0.7 mmHg increase (White et al., 2021).
That subgroup difference matters clinically. If your blood pressure is already elevated or you are on antihypertensive drugs, Jatenzo's BP effect may be more pronounced. The FDA label requires blood pressure measurement before starting Jatenzo, during treatment, and after stopping. Jatenzo is contraindicated in men with uncontrolled hypertension.
To put the 3–5 mmHg figure in context: a sustained systolic increase of that magnitude increases stroke risk meaningfully at the population level, but at an individual level the absolute risk depends heavily on your starting cardiovascular risk. For a healthy 40-year-old with normal blood pressure, a 3 mmHg systolic increase is unlikely to be clinically significant. For someone with existing cardiovascular disease or stage 2 hypertension, the calculus changes.
This is not a reason to avoid Jatenzo outright. It is a reason to take the monitoring protocol seriously.
How Does Jatenzo Compare to Injections and Gels?
Jatenzo achieves comparable testosterone restoration to injections and gels — 84–87% of men reach the eugonadal range — but differs substantially in how it is administered and what risks require monitoring. Every TRT form trades something; with Jatenzo, the trade is needles and transfer risk for food-timing discipline and a blood pressure signal that must be tracked.
Versus injections (cypionate, enanthate): Injections are typically given every one to two weeks intramuscularly, or every seven to ten days subcutaneously for a smoother curve. They produce well-characterized peaks and troughs that many clinicians and patients learn to manage. They are cost-effective and do not require food timing. The downside is the injection itself, the supraphysiological peak in the first days after injection, and the low-T trough before the next dose. Jatenzo provides twice-daily dosing that more closely mimics diurnal variation, though it does require consistent meal timing and fat content.
Versus topical gels and creams: Gels and creams offer flexible dosing and no needles, but they require daily application to clean skin, gloves to prevent transfer, and careful attention to coverage sites. Transfer to partners or children is a documented risk. Jatenzo eliminates transfer risk entirely. In the Jatenzo pivotal trial, both oral TU and Axiron topical achieved the same 87% eugonadal rate (Swerdloff et al., 2020), so efficacy is not the differentiator — it is the administration and risk profile.
Versus injectable testosterone undecanoate (Aveed): The names cause real confusion. But these are not interchangeable. Aveed is injectable testosterone undecanoate given as a 3 mL intramuscular injection at the start of therapy, then at four weeks, then every 10 weeks. It requires a 30-minute post-injection observation period in a healthcare setting because of the risk of pulmonary oil microembolism and anaphylaxis. Jatenzo is a daily oral capsule. Same active molecule, opposite administration, different risk profiles.
Patient satisfaction data: An open-label single-arm trial in which hypogonadal men were switched to Jatenzo from their previous testosterone therapy found significant improvements across all Treatment Satisfaction Questionnaire for Medication (TSQM-9) scores over six months, with stable symptom control on the qADAM questionnaire and no clinically significant changes in hematocrit or PSA (Rivero et al., 2024). A related earlier study found that men switching to oral TU from other forms reported greater satisfaction compared to their prior modalities (Reddy et al., 2023).
For men who are dissatisfied with their current TRT route — needle aversion, gel messiness, transfer concerns — the switch data shows Jatenzo delivers comparable testosterone restoration with higher reported satisfaction.
Other Safety Signals Worth Knowing
Beyond blood pressure, Jatenzo shares most of the standard TRT class-effect safety profile — with one notable exception: it does not cause liver toxicity, because the drug never takes the portal route.
No hepatotoxicity. Jatenzo produced no clinically significant liver enzyme abnormalities across any of the phase III trials — a direct result of the lymphatic absorption route that eliminates hepatic first-pass exposure. This separates it cleanly from older oral androgens where liver damage was a real risk.
Hematocrit elevation. Like all forms of testosterone replacement therapy, Jatenzo can raise red blood cell production. In the two-year study, hematocrit increased but stayed below 48% throughout (Honig et al., 2022). Hematocrit should be monitored as part of standard TRT follow-up regardless of the delivery form.
DHT elevations. Oral testosterone undecanoate produces dihydrotestosterone (DHT) elevations during systemic hydrolysis. A crossover study examining finasteride co-administration with oral TU found that DHT was elevated but, unusually, finasteride did not significantly reduce DHT levels — suggesting the lymphatic route of absorption alters the 5-alpha reductase response compared to other formulations (Roth et al., 2011). The clinical significance of elevated DHT for BPH symptoms or hair loss at approved therapeutic doses remains unclear.
Spermatogenesis suppression. Like all exogenous testosterone, Jatenzo suppresses LH and FSH, which suppresses sperm production. This is a class effect, not specific to the oral route. Men who want to preserve fertility should discuss this before starting any TRT. The broader question of how testosterone therapy affects long-term health is worth understanding before committing to any form.
Schedule CIII controlled substance. All testosterone products fall under Schedule III of the Controlled Substances Act. Specific prescribing rules apply — no refills on a single script in most states.
Oral Testosterone Undecanoate: US-Approved Options
| Feature | Jatenzo | Kyzatrex | Tlando |
|---|---|---|---|
Who Is Jatenzo Approved For?
Jatenzo is FDA-approved for adult men with primary hypogonadism (testicular failure) or hypogonadotropic hypogonadism (pituitary or hypothalamic dysfunction) — the two classic forms of clinical testosterone deficiency.
Diagnosis requires two separate morning testosterone measurements below the normal range, drawn on different days, in the presence of signs and symptoms. In clinical practice, this two-draw requirement exists because testosterone levels fluctuate — a single low reading can be a lab artifact or stress-related suppression rather than true hypogonadism. Both draws must be below range before prescribing is appropriate. Age-related testosterone decline alone — sometimes called "late-onset hypogonadism" — is not a labeled indication, consistent with the broader TRT label context (Campbell et al., 2023).
Men with uncontrolled hypertension should not use Jatenzo. Men with a history of or risk factors for prostate carcinoma or breast carcinoma are contraindicated from all androgen therapies. Standard TRT contraindications apply.
Two other oral testosterone undecanoate formulations — Kyzatrex (approved 2022) and Tlando (approved 2022) — are available in the US and work by the same lymphatic absorption mechanism, as reviewed by Bhat & Dobs (2022). They differ in specific formulation and dose ranges. For a side-by-side look at how these and other TRT forms stack up, see our guide to testosterone replacement therapy options. Your prescriber can advise on which formulation suits your clinical picture.
What Does HEXIS Do Differently?
At HEXIS, oral testosterone isn't a one-size decision. Your protocol starts with a full hormone panel — not a guess — and accounts for your blood pressure history, metabolic picture, and lifestyle before any prescription is written. If Jatenzo is the right fit, your provider will walk you through the food-timing requirements, the BP monitoring schedule, and what follow-up labs actually need to look like.
If you want a physician who thinks through your full picture, schedule a consultation and we will start with your numbers.
Frequently Asked Questions
Does Jatenzo work as well as testosterone injections?
Phase III trial data shows Jatenzo restores testosterone to the eugonadal range in 84–87% of hypogonadal men, comparable to topical formulations (Swerdloff et al., 2020). Direct head-to-head comparison against cypionate or enanthate injections has not been published, but efficacy in reaching target testosterone levels is similar across approved TRT formulations when properly titrated.
What happens if I take Jatenzo without food?
Absorption drops dramatically. In pharmacokinetic studies, testosterone AUC with a near-fasting meal (0.6 g fat) was 30.7 nmol·h/L versus 146 nmol·h/L with a 19-gram fat meal — roughly a five-fold difference (Schnabel et al., 2007). Taking Jatenzo without adequate dietary fat significantly undermines its effectiveness. Every dose requires a meal with at least 19 grams of fat.
Is Jatenzo the same as Aveed?
No. Both contain testosterone undecanoate, but they are entirely different products. Aveed is an intramuscular injection given in a healthcare setting every 10 weeks. Jatenzo is a twice-daily oral capsule. The routes, risk profiles, and prescribing logistics are distinct — the shared molecule is the only similarity.
How is blood pressure monitored on Jatenzo?
The FDA label requires BP measurement before starting Jatenzo, at regular intervals during treatment, and after stopping. If systolic blood pressure rises or hypertension becomes uncontrolled, Jatenzo should be discontinued. Men who are already on antihypertensive therapy tend to see larger BP increases — 3.4 mmHg versus 0.7 mmHg in non-medicated men — so monitoring frequency may need to increase in that group (White et al., 2021).
Can Jatenzo affect the liver?
No hepatotoxicity was observed across the Jatenzo phase III program. This is mechanistically expected: because testosterone undecanoate is absorbed via intestinal lymphatics rather than the portal vein, it bypasses hepatic first-pass metabolism and does not require the 17-alpha alkylation that made older oral androgens liver-toxic (Patel et al., 2022).
This article is for informational purposes only and does not constitute medical advice. HEXIS Health is a physician-led TRT clinic. Always consult a qualified healthcare provider before starting, stopping, or modifying any testosterone therapy.
- 1
Jatenzo is the first FDA-approved oral testosterone for hypogonadism — it works by absorbing through intestinal lymphatics, bypassing the liver entirely. No hepatotoxicity risk.
- 2
It restores testosterone to the normal range in 84–87% of hypogonadal men in phase III trials, with efficacy sustained at 24 months.
- 3
The FDA boxed warning on blood pressure is real — systolic BP rises 3–5 mmHg on average, more if you are already on antihypertensives. Monitoring is mandatory.
- 4
Taking it without food (or with too little fat) reduces absorption by roughly five-fold. Every dose needs a meal with at least 19 grams of fat.
- 5
Jatenzo and Aveed both contain testosterone undecanoate but are entirely different products — Aveed is a 10-week injection, Jatenzo is a daily capsule.