What Low Testosterone Does to Your Body: A System-by-System Breakdown
What Low Testosterone Does to Your Body: A System-by-System Breakdown
Understanding what low testosterone does to your body changes how you look at a lot of symptoms that doctors tend to brush off. The fatigue. The soft middle. The mood that's been flat for two years. The motivation that quietly left.
Low testosterone does not just affect your sex drive. It affects seven distinct body systems — and in many men, several of them are already in trouble by the time someone thinks to run a hormone panel.
Here is what the research actually shows, system by system.
The short answer: Low testosterone — clinically defined as total testosterone below 300 ng/dL on two morning fasting draws — affects sexual function, body composition, bone density, mood, metabolism, cardiovascular health, and red blood cell production. Most of these effects are at least partially reversible with medically supervised treatment.
How Does Low Testosterone Affect Sexual Function?
Low testosterone impairs three distinct sexual domains simultaneously: libido, erectile function, and sexual activity frequency — and most men do not realize these are separate mechanisms until they are all affected at once.
The TRAVERSE sexual function substudy confirmed this across 5,204 men with confirmed hypogonadism. Men on testosterone showed meaningful improvements in all three domains versus placebo (Pencina et al., 2024) — making this the largest controlled evidence base for TRT's effect on sexual function.
Libido — or more accurately, the absence of it — is often the first thing men notice. Not a gradual slowdown, but a flat indifference that feels qualitatively different from a bad week. Erectile function is a separate mechanism: testosterone influences nitric oxide signaling in penile tissue, and when levels drop, the hydraulics become unreliable even when desire is present. Frequency of sexual activity tends to follow both.
The review literature backs this up. Testosterone replacement therapy has consistently shown benefits for sexual symptoms in men with confirmed hypogonadal levels — with effect sizes strongest when baseline T is genuinely low, not just in the lower-normal range (Rastrelli et al., 2019).
If you want a deeper look at the full spectrum of symptoms that low testosterone produces — including the sexual ones — see our guide to low testosterone symptoms.
What Does Low Testosterone Do to Body Composition?
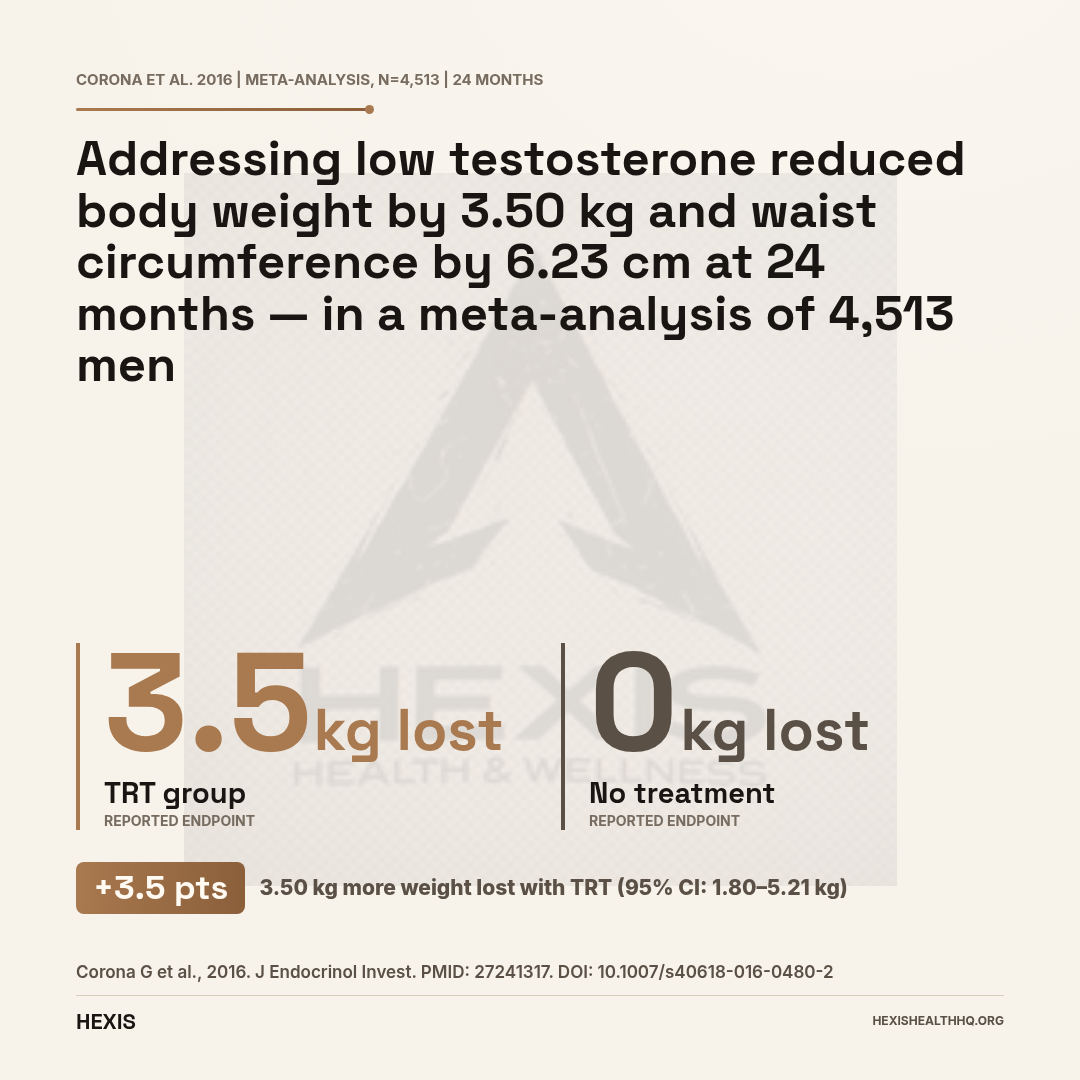
Low testosterone directly drives both muscle loss and fat gain — and a meta-analysis of 4,513 men found that addressing the deficiency reversed both, with body weight falling 3.50 kg and waist circumference shrinking 6.23 cm at 24 months (Corona et al., 2016). What many men blame on aging is often hormonal.
The confidence intervals on those changes were tight — 95% CI −5.21 to −1.80 kg for weight and −7.94 to −4.76 cm for waist — meaning the effect was consistent across the population of 4,513 men studied, not driven by a subset of extreme responders.
The mechanism runs in both directions. Testosterone promotes protein synthesis in muscle and suppresses fat storage, particularly visceral fat. But the relationship between testosterone and obesity is bidirectional: fat tissue converts testosterone into estrogen through a process called aromatization — so more visceral fat means more conversion, which means lower testosterone, which means more fat. Low testosterone can accelerate this cycle (Tsutsumi & Tsuchiya, 2025).
This is why weight loss and testosterone are so closely intertwined in research. Fixing one often helps the other — but in men with true hypogonadism, the cycle may not self-correct.
For a detailed look at what testosterone actually does to muscle, including the specific trial data on lean mass, see our article on whether testosterone builds muscle.
55% higher fracture rate in untreated men
In a 2026 SR/MA of 2,711 hypogonadal men (2 RCTs), those not receiving TRT had a relative risk of 1.55 (95% CI: 1.21–1.97) for clinical fractures compared to TRT-treated men.
Source: Anagnostis et al., 2026. Maturitas. PMID: 42066666
What Happens to Your Bones When Testosterone Is Low?
Low testosterone accelerates bone loss in men — and untreated hypogonadal men face a clinically meaningful fracture risk that most patients and many clinicians underestimate, because osteoporosis has long been framed as a women's condition.
Testosterone supports bone mineral density directly, and men who are testosterone-deficient lose bone faster than their eugonadal peers. In a 2026 systematic review and meta-analysis of two randomized controlled trials (n=2,711 men), men receiving TRT had significantly fewer clinical fractures — a relative risk of 1.55 (95% CI: 1.21–1.97) for the untreated control group (Anagnostis et al., 2026).
That number means untreated hypogonadal men had a 55% higher rate of clinical fractures than those on treatment. For a condition most men do not associate with broken bones, that is a meaningful signal.
TRT improves bone mineral density at the lumbar spine and hip — the two sites most relevant to fracture outcomes. The improvement is clearest when treatment starts before severe bone loss has occurred. Hypogonadal men should consider bone density screening, particularly if they have had low testosterone for several years without treatment (Barbonetti et al., 2020).
How Does Low Testosterone Affect Mood, Cognition, and Energy?
Low testosterone produces measurable depressive symptoms in a significant share of hypogonadal men — and in the TRAVERSE depression substudy, TRT produced significantly greater PHQ-9 improvement than placebo in men who had never been diagnosed with a mood disorder (Bhasin et al., 2024).
The men enrolled had PHQ-9 scores above 4 — not severe clinical depression, but the kind of low-grade persistent flatness that is easy to dismiss as stress or aging. That is the population where the TRT benefit was demonstrated, which makes it directly relevant to the men most likely to be reading this.
The cognitive picture is more complicated. There is mechanistic evidence for testosterone's role in brain function — the hormone has receptors in regions involved in memory and executive function — but the randomized trial data on cognitive outcomes is less definitive than the mood data. What the trials consistently show is that energy, fatigue, and motivation respond to TRT in hypogonadal men.
The practical point: if you have been "fine" but not really fine for a while — tired despite adequate sleep, unmotivated, flat — and your testosterone has never been measured, that is a data gap worth closing.
Low Testosterone and Metabolic Health: The Insulin Resistance Connection
Low testosterone and metabolic disease are bidirectionally associated — they promote each other, and separating cause from effect is difficult in observational data.
Men with low testosterone have higher rates of insulin resistance, metabolic syndrome, and type 2 diabetes than testosterone-sufficient men. The relationship is not fully explained by obesity, though obesity is a major confounder. There is evidence that testosterone directly supports insulin signaling in skeletal muscle, independent of its effects on body composition (Muraleedharan & Jones, 2014).
The body composition changes that low testosterone drives — reduced lean mass, increased visceral fat — themselves worsen insulin resistance, creating another self-reinforcing cycle. TRT-mediated improvements in body composition (as seen in the Corona et al., 2016 meta-analysis) appear to partly explain the metabolic improvements observed with treatment.
In men with type 2 diabetes or metabolic syndrome who also have confirmed hypogonadism, treating the testosterone deficiency is not optional. It is part of the metabolic management, not a separate aesthetic concern.
For a broader look at symptoms that span multiple systems — including metabolic ones — see our guide on low testosterone symptoms.
TRAVERSE Trial — Cardiovascular Safety (n=5,246)
| Group | MACE Rate | Result |
|---|---|---|
Source: Lincoff et al., 2023. N Engl J Med. PMID: 37326322
What Did the Largest Cardiovascular Trial Show?
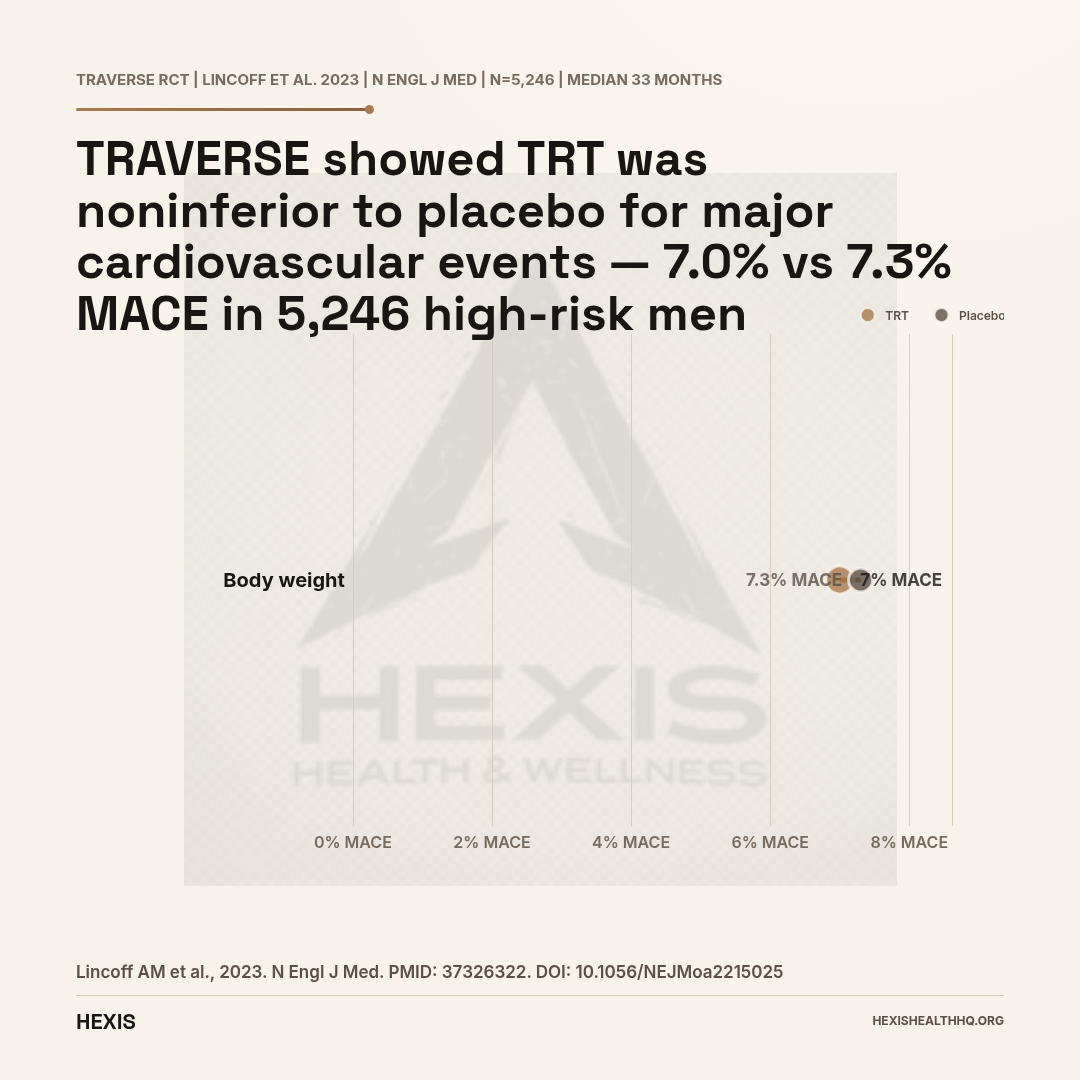
The largest randomized trial on testosterone and heart safety — TRAVERSE, 5,246 men published in the New England Journal of Medicine — found that TRT was noninferior to placebo for major cardiovascular events, with MACE rates of 7.0% versus 7.3% (Lincoff et al., 2023).
TRAVERSE enrolled men with hypogonadism who already had cardiovascular disease or elevated cardiovascular risk — the highest-risk population you would want to study. That population matters: if TRT were going to cause harm, this is where you would have seen it. The noninferiority result — TRT did not increase cardiovascular risk — was the clinically meaningful finding (Lincoff et al., 2023).
This is important framing. Noninferiority is not the same as proven cardiovascular benefit — TRAVERSE was not designed to show TRT prevents heart attacks. It showed TRT did not cause them in men already at elevated risk.
There was one signal from TRAVERSE worth noting: a modestly higher rate of atrial fibrillation in the TRT group. This is something your provider should discuss with you if you have any history of arrhythmia (Lincoff et al., 2023).
Prior observational studies suggested both increased and decreased cardiovascular risk with testosterone — the conflicting findings reflected selection bias and confounding more than true signal. TRAVERSE was the RCT that settled the primary safety question. The association between very low testosterone and poor cardiovascular outcomes in epidemiological data likely reflects the underlying illness burden of severely hypogonadal men, not a direct causative pathway (Goodale et al., 2017).
What Does Low Testosterone Do to Your Blood?
Testosterone has two opposing effects on blood: it can correct anemia by stimulating red blood cell production, and it can cause polycythemia if levels run too high. Both are real, and both require monitoring.
Anemia. Testosterone stimulates erythropoiesis — red blood cell production — through pathways involving erythropoietin and iron utilization. When testosterone is low, red blood cell production can fall, contributing to anemia. In men with chronic kidney disease, testosterone deficiency was associated with a 5.3-fold increase in anemia odds (OR 5.3, 95% CI: 2.2–12.5) compared to testosterone-sufficient men (Carrero et al., 2012). In the T-Trials anemia substudy, testosterone replacement raised hemoglobin by 0.58 g/dL (95% CI: 0.31–0.85 g/dL) in men with unexplained anemia (Artz et al., 2020).
That half a gram of hemoglobin improvement may not sound like much, but in men with borderline anemia — who feel chronically tired and attribute it to age or stress — it is clinically meaningful.
Polycythemia. The flip side: testosterone also carries a risk of driving hemoglobin too high, a condition called polycythemia or erythrocytosis. This is a monitoring issue, not a reason to avoid TRT — but hematocrit checks are a non-negotiable part of responsible TRT management. Most clinics flag hematocrit above 54% as the threshold for dose adjustment or temporary hold (Di Lodovico et al., 2022).
Testosterone's effect on blood is dose- and delivery-dependent. Injectable testosterone carries a higher erythrocytosis risk than transdermal formulations, which is one reason delivery route matters in individualized treatment decisions.
When Should You Get Evaluated — and Are the Effects Reversible?
The Endocrine Society's 2018 Clinical Practice Guideline specifies that hypogonadism should be diagnosed with two morning, fasting testosterone measurements below 300 ng/dL, combined with symptoms consistent with testosterone deficiency (Bhasin et al., 2018). One measurement is not enough — testosterone varies significantly by time of day, recent illness, and acute stress.
The 300 ng/dL cutoff is a clinical threshold, not a biological cliff. Some men feel symptoms at 400 ng/dL; others function fine at 280. The symptom picture matters as much as the number.
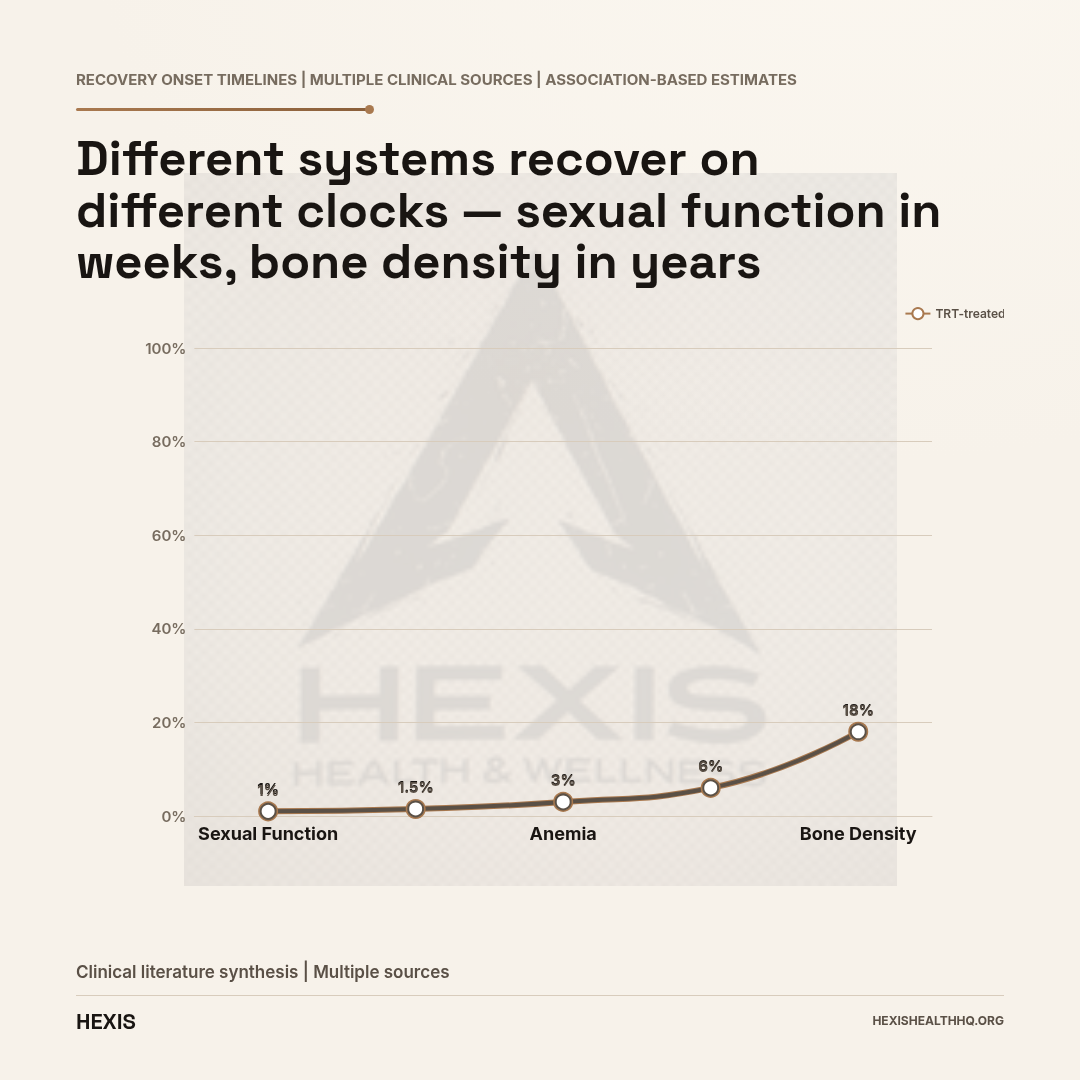
Recovery timelines by system — most effects are at least partially reversible with medically supervised TRT:
- Sexual function responds within 3–6 weeks and continues improving through 3 months.
- Body composition changes emerge over 3–6 months and continue for 12–24 months.
- Bone mineral density improves measurably over 12–24 months of treatment.
- Mood and energy often respond within 4–6 weeks.
- Anemia from low T responds within 3 months of treatment.
How fully these effects reverse depends on how long levels have been low, age at treatment, and baseline health. Earlier treatment generally produces more complete recovery.
If you are exploring what treatment actually looks like — the delivery methods, monitoring protocols, and what to expect — our guide to how to treat low testosterone covers the clinical options in detail.
If you think your testosterone may be low and you want real numbers instead of a guess, HEXIS starts with bloodwork — not a questionnaire. Schedule a consultation and your provider will review your full hormone panel before any conversation about treatment.
Frequently Asked Questions
What is the most common symptom of low testosterone?
Fatigue is the most commonly reported symptom, followed closely by reduced libido and difficulty building or maintaining muscle. Many men report all three simultaneously before realizing they share a single hormonal cause. The overlap between low testosterone symptoms and general stress or aging makes hypogonadism easy to miss without lab testing.
Does low testosterone cause depression?
Low testosterone is associated with depressive symptoms, particularly low mood, reduced motivation, and flat affect — sometimes called dysthymia or persistent depressive disorder. In the TRAVERSE trial, hypogonadal men with elevated depression scores showed greater symptom improvement on TRT than on placebo (Bhasin et al., 2024). However, low testosterone is not the only cause of depression, and the two conditions are not interchangeable.
Can low testosterone go undetected for years?
Yes. Many symptoms of hypogonadism — fatigue, weight gain, brain fog, reduced libido — are common enough to be attributed to stress, poor sleep, or simply getting older. Without a fasting morning testosterone test, the diagnosis is frequently missed. Men often report that symptoms had been present for two to five years before testing revealed a problem.
Is low testosterone dangerous long-term?
Sustained untreated hypogonadism is associated with bone loss, body composition deterioration, insulin resistance, and reduced quality of life. The fracture data from Anagnostis et al. (2026) shows a 55% higher fracture rate in untreated hypogonadal men compared to those receiving TRT — a clinically significant long-term consequence. Cardiovascular risk with low testosterone appears to be associational rather than directly causative, but the co-morbidity burden in severely hypogonadal men is real.
How quickly do you feel better after starting testosterone treatment?
Sexual function and mood typically show improvement within 3–6 weeks for most men. Energy and motivation often respond within the first month. Body composition changes — meaningful shifts in muscle and fat — generally take 3–6 months to become visible, and continue improving for 12–24 months. Bone density changes are the slowest, measurable at 12–24 months with DEXA scan.
- 1
Sexual function and mood: improvement begins in 3–6 weeks
- 2
Body composition: visible changes at 3–6 months, continuing through 24 months
- 3
Bone mineral density: measurable gains at 12–24 months
- 4
Anemia: responds within 3 months of treatment
- 5
Diagnosis requires two fasting morning T draws below 300 ng/dL plus symptoms