AndroGel: Uses, Dosing and Alternatives
AndroGel: Uses, Dosing and Alternatives
AndroGel is a prescription testosterone gel applied daily to the skin — it's one of the most widely prescribed forms of testosterone replacement therapy in the United States. If your doctor just handed you a prescription for it, or you're trying to figure out whether it's the right TRT option for you, this is the breakdown you need: what it actually does, how the dosing works, what the real safety data looks like, and what the alternatives are if it doesn't fit your situation.
The short answer: AndroGel is FDA-approved for male hypogonadism (low testosterone). It comes in two concentrations — 1% and 1.62% — applied once daily to the shoulders, upper arms, or abdomen. The 5,204-person TRAVERSE trial used the 1.62% formulation and confirmed cardiovascular non-inferiority versus placebo in men with existing heart disease risk. Skin-to-skin transfer to women and children is the primary safety concern requiring precautions.
What Is AndroGel Used For?
AndroGel is FDA-approved specifically for male hypogonadism — a condition where the testes don't produce enough testosterone on their own. That covers two categories: primary hypogonadism (the problem is in the testes themselves, from causes like injury, infection, or Klinefelter syndrome) and hypogonadotropic hypogonadism (the problem is in the pituitary or hypothalamus failing to signal the testes properly).
The diagnosis requires confirmed low levels — not a single borderline reading. Per the TRAVERSE trial eligibility criteria, that means two separate morning testosterone measurements below 300 ng/dL (Bhasin et al., 2023). The Endocrine Society and American Urological Association both use this threshold. If your doctor called your levels "fine" but didn't give you the number, ask for the actual value.
The symptoms of hypogonadism that TRT addresses include fatigue, reduced libido, erectile dysfunction, loss of lean muscle mass, increased body fat, and mood changes including depression. In the TRAVERSE sub-study analyzing depressive syndromes in hypogonadal men, participants who received testosterone replacement therapy showed significant improvement compared to placebo (Bhasin et al., 2024). The effect is real, but it's not universal — testosterone doesn't fix depression that isn't driven by low T.
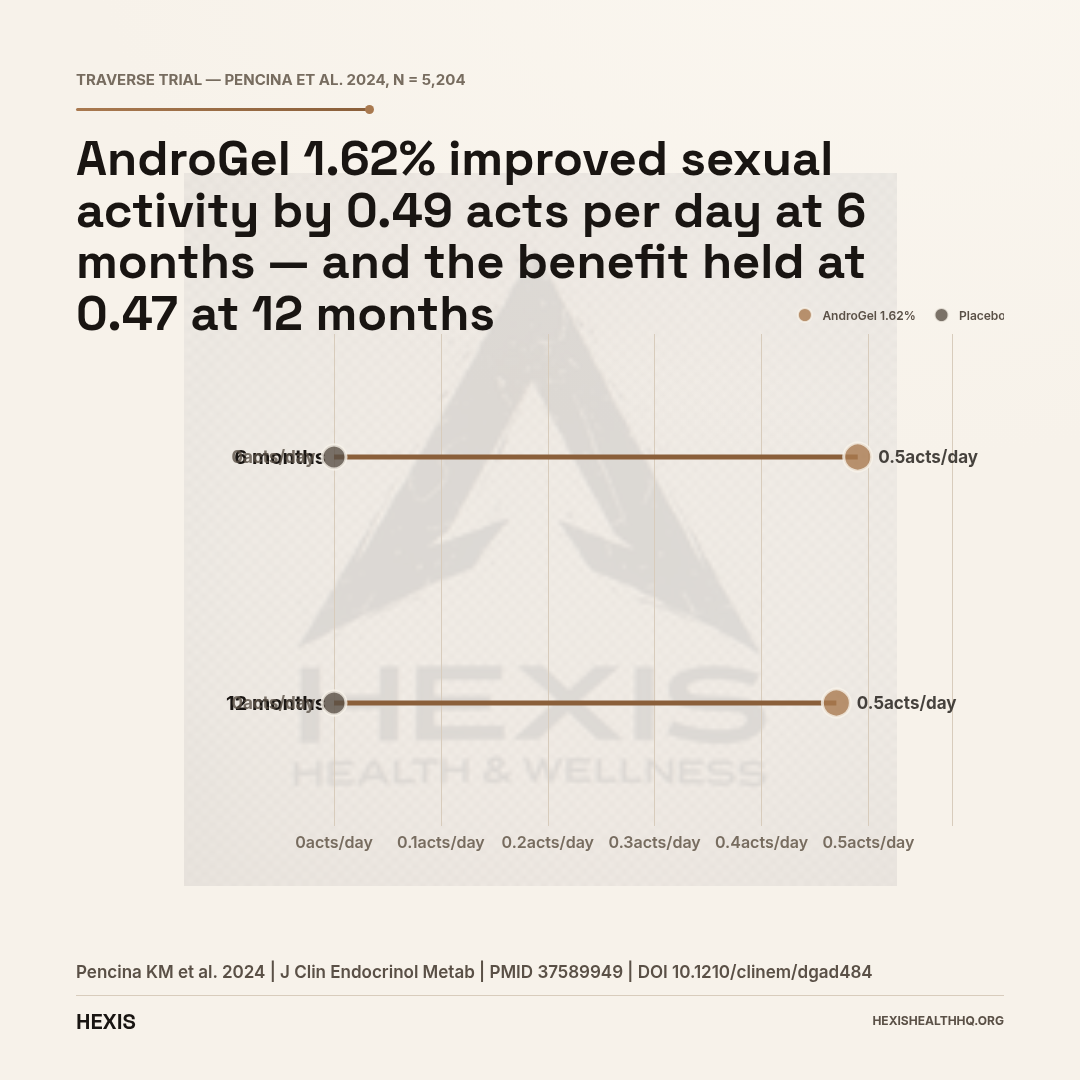
For sexual function specifically, the TRAVERSE data showed that men on 1.62% testosterone gel reported an improvement of 0.49 sexual acts per day at six months and 0.47 acts per day at twelve months compared to placebo (Pencina et al., 2024). That's a meaningful, sustained benefit — not a placebo response.
Late-onset hypogonadism (age-related testosterone decline) is a distinct category. The diagnosis and treatment approach requires ruling out reversible causes first, because functional hypogonadism driven by obesity, sleep apnea, or metabolic syndrome can often be addressed without TRT (Foresta et al., 2015).
AndroGel 1% vs AndroGel 1.62%
| AndroGel 1% | AndroGel 1.62% | |
|---|---|---|
Source: Bhasin et al., 2023 — PMID 38150256
AndroGel 1% vs 1.62%: What Is the Difference?
AndroGel comes in two distinct FDA-approved formulations that are not interchangeable dose-for-dose — the concentration affects both your daily volume and the titration schedule your provider will use.
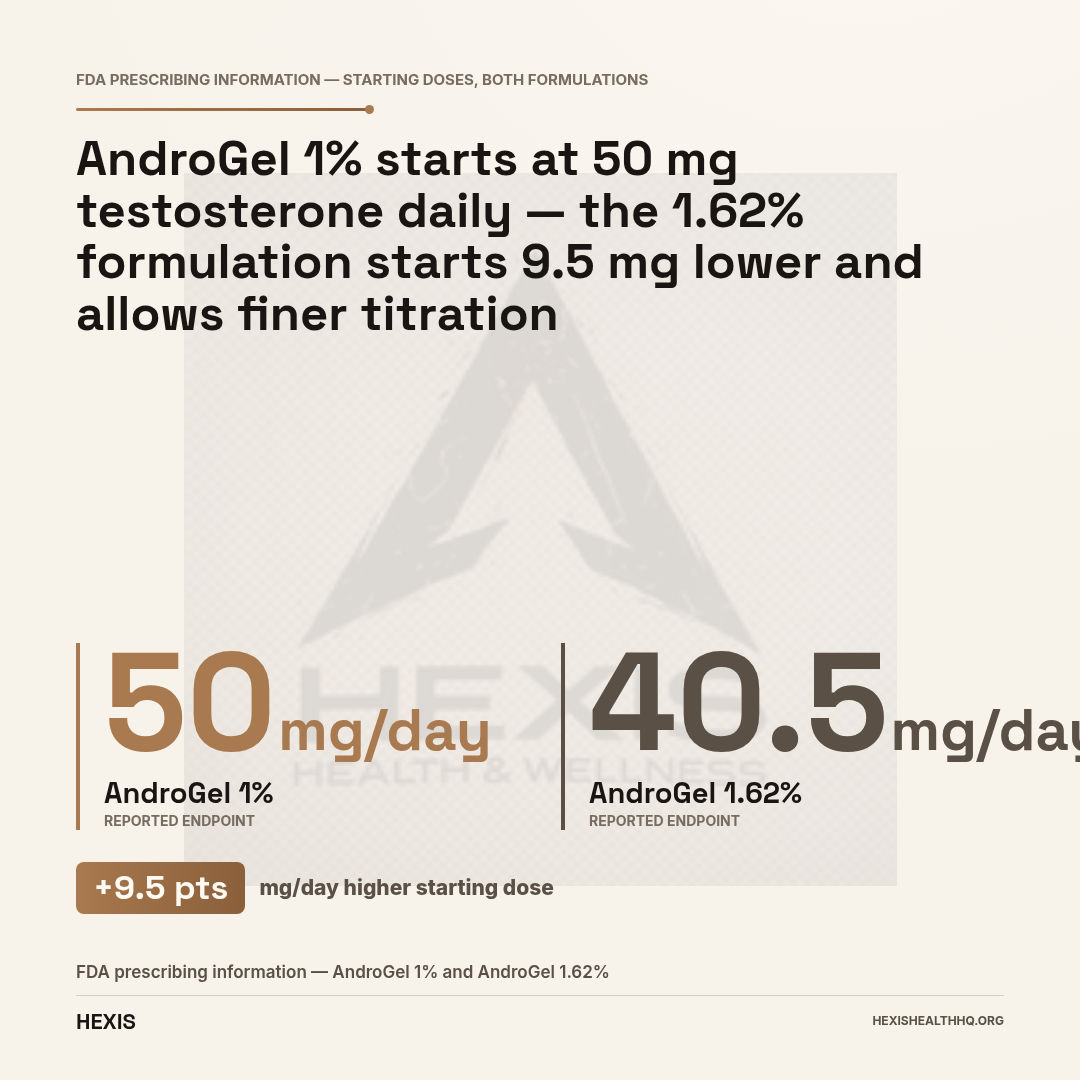
AndroGel 1% is dispensed as a pump that delivers 1.25 g of gel (12.5 mg testosterone) per actuation. The starting dose is typically 5 g daily (two pumps, delivering 50 mg testosterone). After two weeks, if serum testosterone remains below the target range, the dose can be increased to 7.5 g or 10 g daily.
AndroGel 1.62% delivers 20.25 mg of testosterone per 1.25 g actuation. The starting dose is 40.5 mg (two actuations) applied daily to the upper arms and shoulders. After 14 days of use, the dose can be adjusted based on serum testosterone levels — down to one pump (20.25 mg) or up to four pumps (81 mg) daily. The 1.62% formulation is what was used throughout the landmark TRAVERSE trial (n = 5,204), which means the strongest long-term safety data we have for topical testosterone gel applies specifically to this concentration (Bhasin et al., 2023).
For the 1.62% gel, approved application sites are the upper arms and shoulders only — not the abdomen. Rotate between left and right sides. Apply after showering, let dry completely before dressing, and wash hands thoroughly with soap and water immediately after application.
Men who switched between AndroGel and Testim (another testosterone gel) for suboptimal responses showed that switching formulations can improve levels when one preparation isn't working adequately (Grober et al., 2008). If your levels aren't reaching the target range at your current dose, changing gel products or formulations is an option worth discussing with your provider before jumping straight to injections.
What Does the TRAVERSE Trial Tell Us About Safety?
TRAVERSE answered the cardiovascular safety question that had stalled TRT prescribing for years — and the answer, for a high-risk population, was that testosterone gel did not increase the rate of major cardiac events.
The TRAVERSE trial (NCT03518034) enrolled 5,204 men aged 45 to 80 with confirmed hypogonadism and existing cardiovascular disease or elevated cardiovascular risk. It was a randomized, double-blind, placebo-controlled trial using AndroGel 1.62% as the active intervention. This is the largest and most rigorously designed TRT safety trial ever completed.
Cardiovascular outcomes: Testosterone replacement therapy was non-inferior to placebo for major adverse cardiovascular events — meaning the gel did not increase the risk of heart attack, stroke, or cardiovascular death compared to placebo in this high-risk population (Bhasin et al., 2023). For men who had been warned off TRT because of cardiovascular concerns, this is a significant finding.
Prostate safety: The TRAVERSE prostate sub-study found no statistically significant increase in high-grade prostate cancer incidence in men on TRT versus placebo (Bhasin et al., 2023). Baseline PSA in enrolled participants was 0.92 ng/mL (SD 0.67). There was a small increase in benign prostatic hyperplasia events and prostate biopsy rates in the TRT group, which is consistent with testosterone's known effect on prostate tissue — but the feared cancer signal did not materialize. Men with active or suspected prostate cancer remain an absolute contraindication.
Depressive symptoms: Among TRAVERSE participants who had depressive syndromes at baseline, testosterone replacement produced significant improvement versus placebo (Bhasin et al., 2024). This wasn't a primary endpoint of the main trial, but the sub-study results are clinically meaningful.
The cardiovascular picture is not perfectly clean — erythrocytosis (elevated red blood cell count) and atrial fibrillation both occurred at higher rates in the TRT group. Your provider needs to monitor for these, not just reassure you that the main MACE numbers were clean.
Skin-to-Skin Transfer: The REMS Warning
The FDA-mandated Risk Evaluation and Mitigation Strategy (REMS) for testosterone gels exists because of skin-to-skin transfer risk — the gel can transfer from your skin to another person's skin through direct contact before it fully dries.
This matters most for women and children. In women, accidental testosterone exposure causes virilization — facial hair, voice changes, clitoral enlargement. In children, exposure can cause premature puberty. These are not theoretical concerns; they drove the FDA's black box warning that still appears on all testosterone gel labeling.
The practical protocol to minimize transfer risk:
- Apply the gel to covered body areas (upper arms, shoulders) rather than exposed skin
- Let the gel dry completely before putting on a shirt — typically 5 minutes
- Wash hands thoroughly with soap and water after applying
- Cover the application site with clothing before any skin-to-skin contact with women or children
- If contact does occur, have the other person wash the area with soap and water immediately
- Consider showering before any close physical contact if the gel hasn't fully absorbed
If you have young children in the home or a female partner who shares a bed, the transfer protocol is not optional — it's the primary safety behavior the REMS was designed to enforce.
Testosterone gel can transfer to women and children through direct skin contact before drying. In women, exposure causes virilization (facial hair, voice changes). In children, it triggers premature puberty. The FDA mandates a Risk Evaluation and Mitigation Strategy (REMS) for all testosterone gels because of this risk.
Source: FDA REMS Program — Testosterone Gel Products
Monitoring While on AndroGel
Getting the dose right on AndroGel requires lab follow-up — this isn't a prescription you pick up once and never think about again. The monitoring schedule matters for both efficacy and safety, and most men need at least one dose adjustment in the first few months.
Testosterone levels: Check serum total testosterone 14 days after starting or after any dose adjustment. The timing of the draw matters — collect 2 to 8 hours after the morning application to capture the representative level. For AndroGel 1.62%, the target range is typically 400–700 ng/dL, but your provider will individualize this based on your symptoms and baseline.
Hematocrit: Testosterone stimulates red blood cell production by increasing erythropoietin. If hematocrit climbs above 54%, the dose needs to be reduced or stopped temporarily. Men on TRT face an elevated risk of polycythemia, which increases blood viscosity and clotting risk (Chin-Yee et al., 2017). Blood donation is one strategy used to manage elevated hematocrit — though it comes with its own considerations around iron status and eligibility.
PSA: Check at baseline and at regular intervals during treatment. Any rapid rise in PSA warrants evaluation. A confirmed PSA above 4 ng/mL or a rapid rise should prompt urology referral before continuing TRT.
Blood pressure: Testosterone can raise blood pressure. Monitor periodically, especially in men with hypertension. The FDA label specifies that testosterone products are not recommended for use in men with uncontrolled hypertension.
How Does AndroGel Compare to Other TRT Options?
AndroGel differs from other TRT options primarily on cost, transfer risk, and level stability — injections cost less and carry no household transfer risk, while nasal gels preserve fertility better, and pellets eliminate daily dosing (Barbonetti et al., 2020).
Testosterone injections (cypionate or enanthate): Injected intramuscularly or subcutaneously every 1–2 weeks. The big advantage is lower cost — generic testosterone cypionate is significantly cheaper than brand-name AndroGel — and no transfer risk. The tradeoff is the peak-and-trough pattern: testosterone is high the day after injection and falls toward the end of the interval, which some men feel as energy and mood fluctuations. Weekly or twice-weekly injections smooth this out at the cost of more frequent administration.
Natesto (nasal gel): Testosterone delivered intranasally three times daily. It largely avoids suppression of the hypothalamic-pituitary axis because of its short-acting, pulsatile absorption profile, which makes it an option for men who want to preserve fertility (Ide et al., 2020). It requires three daily doses, which affects adherence.
Testim and Fortesta (other topical gels): Same mechanism as AndroGel, different delivery vehicles. Testim is applied to the upper arms and shoulders, while Fortesta is applied to the inner thighs. Switching between gel brands has been used to improve levels in men who aren't reaching their target on one product (Grober et al., 2008).
Subcutaneous pellets (Testopel): Pellets implanted under the skin every 3 to 6 months, delivering a steady dose without daily application. The upside is convenience — no daily routine, no transfer risk. The downside is that dose adjustments require a clinical procedure, and extrusion and infection at the implant site are known complications.
Buccal testosterone (Striant): Absorbed through the gum tissue. Applied twice daily. Largely replaced by other options due to adherence challenges and gum irritation.
The choice between these options depends on cost, your household situation (children, female partner), fertility goals, how reliably you'll follow a daily protocol, and your preference for how much level stability you want (Tsametis et al., 2018).
What Should You Expect When Starting AndroGel?
Testosterone gel takes longer to produce noticeable results than most men expect — and the most common reason patients question whether it's working is that they haven't had their levels checked at the 14-day mark to confirm the dose is actually in range.
Sexual function typically improves within 3 to 6 weeks. Energy and mood often shift within 3 to 4 weeks. Body composition changes — gaining lean mass, losing fat — take 3 to 6 months of consistent treatment, and full benefit at a steady dose may not be apparent for 12 months (Barone et al., 2022). Bone density effects, if relevant, take 1 to 2 years.
The first 14 days matter for dose calibration — this is when your lab check happens to see if the starting dose is putting your levels in the target range. If you feel nothing after 4 to 6 weeks, that's the signal to check whether levels are actually in range before concluding that TRT doesn't work for you.
Some men are genuinely non-responders to topical gel because of poor skin absorption. Absorption varies significantly by application site, skin hydration, and individual skin characteristics. If your serum testosterone isn't rising adequately despite dose increases, switching delivery method rather than continuing to push the gel dose is a reasonable step (Giagulli et al., 2011).
Frequently Asked Questions
Can AndroGel increase testosterone to normal levels?
Yes, for most men. In the TRAVERSE trial, participants on 1.62% testosterone gel achieved serum levels consistent with normal male range. The starting dose achieves target levels in many men, but some require titration upward. If levels remain below 400 ng/dL at the maximum approved dose, your provider may switch you to an injection-based protocol, which delivers testosterone more directly into the bloodstream.
Is AndroGel safe for men with heart disease?
The TRAVERSE trial was specifically designed for men with cardiovascular disease or elevated risk, and TRT was cardiovascular non-inferior to placebo at 33 months of follow-up (Bhasin et al., 2023). That means the gel did not increase the rate of heart attack, stroke, or cardiovascular death in that population. However, erythrocytosis and atrial fibrillation were more common on TRT, so men with heart disease need close monitoring.
Does AndroGel affect fertility?
Yes — exogenous testosterone suppresses the pituitary signals (LH and FSH) that drive sperm production. Most men on AndroGel will experience reduced or absent sperm production while using it. If fertility preservation is a goal, nasal testosterone (Natesto) or clomiphene-based protocols are typically recommended instead, since they work differently and are less suppressive of natural testicular function (Ide et al., 2020).
How long does it take for AndroGel to work?
Sexual function and libido improvements often appear within 3 to 6 weeks. Energy and mood may shift in 3 to 4 weeks. Lean body mass changes take 3 to 6 months, with full body composition benefit at 12 months. Checking your levels at 14 days confirms whether the starting dose is getting you into range — if it isn't, dose adjustment happens then, not after waiting months.
What happens if I stop using AndroGel?
Your testosterone levels will return to their pre-treatment baseline within a few weeks of stopping. The symptoms of hypogonadism — fatigue, low libido, mood changes — typically return as well. Stopping abruptly is not dangerous, but the underlying hypogonadism is still present. There is no permanent restoration of natural testosterone production from TRT; the gel replaces what the body isn't producing but doesn't fix the underlying cause.
Working With a Provider on TRT
If you're looking at AndroGel, the conversation with your provider should start with labs — not a prescription. Two morning testosterone draws below 300 ng/dL are required for diagnosis. After that, a full panel matters: total testosterone, free testosterone, LH, FSH, SHBG, hematocrit, PSA, and a metabolic panel. These labs tell you not just whether your testosterone is low, but why — and whether there are contraindications to treatment.
At HEXIS, we build TRT protocols around your specific numbers, not a generic starting dose. If you want to know what your labs look like and whether testosterone replacement makes sense for your situation, Schedule a consultation.
For more context on testosterone replacement therapy broadly, see our guide on testosterone replacement therapy. If you're trying to understand whether your labs point to a real problem, low testosterone symptoms explains what the numbers actually mean. For men weighing topical gel against weekly shots, our injectable testosterone guide covers the injection protocols in detail.
- 1
Requires two morning testosterone readings below 300 ng/dL to diagnose hypogonadism — one normal reading doesn't rule it out.
- 2
The 1.62% formulation has the strongest long-term safety data from TRAVERSE (n = 5,204): cardiovascular non-inferior to placebo, no increase in high-grade prostate cancer.
- 3
Skin-to-skin transfer is the top household safety concern — the REMS protocol is required, not optional.
- 4
Hematocrit above 54% is the main monitoring threshold that triggers dose reduction; check at baseline and follow-up.
- 5
If gel isn't getting your levels into range after titration, switching to injections is straightforward — not a failure.