Best Supplements for Testosterone (Evidence-Based)
Best Supplements for Testosterone (Evidence-Based)
Reviewed by the HEXIS Health Medical Team — clinicians who order and interpret testosterone panels daily.
The short answer: Most testosterone supplements work only in men who have a measurable deficiency — vitamin D, zinc, or magnesium. Outside of that correction mechanism, ashwagandha (KSM-66) has the most consistent RCT evidence for raising testosterone in healthy men: 14.7–18% increases in double-blind trials. Tribulus terrestris and D-aspartic acid consistently fail in rigorous research. No supplement approaches the magnitude of TRT for clinically low testosterone.
Most "testosterone booster" supplements fail to raise testosterone in men who already have normal levels. A handful of specific compounds — ranked here by the strength of their clinical trial evidence — can make a real difference, but almost always by correcting a deficiency, not by supercharging a healthy system. Here's what the clinical research actually shows, supplement by supplement.
Why Most Supplements Disappoint (and Why a Few Don't)
The single most important distinction in testosterone supplement research: deficiency correction is not the same as boosting. Most supplements on the market either correct a nutritional deficit that was suppressing testosterone, or they fail entirely — very few raise testosterone above baseline in men who are already replete and healthy.
Vitamin D, zinc, and magnesium fall into the deficiency-correction category. If your levels are low, restoring them can bring testosterone back to where it belongs. If your levels are already adequate, adding more does nothing measurable for testosterone. That's not a failure of the supplement — it's basic physiology.
Ashwagandha, fenugreek, and tongkat ali are different. These have RCT data in men who weren't deficient in anything specific. They appear to work through other mechanisms — stress-axis modulation, enzyme inhibition, or direct effects on the hypothalamic-pituitary-gonadal axis.
Then there are the supplements that show up in every "top 10" list despite consistently failing in rigorous trials. Tribulus terrestris is the most prominent example.
This article covers each category honestly. For a broader look at whether OTC testosterone boosters work at all — the top-level evidence question — see our testosterone booster guide.
70.0% relative scale
of American adults are vitamin D deficient — the most common nutritional gap behind low testosterone
Does Vitamin D Supplementation Actually Raise Testosterone?
Vitamin D raises testosterone primarily in men who are deficient — in replete men, RCTs consistently show no significant testosterone change. It has the largest research base of any supplement on this list, but that base is almost entirely in deficient populations.
A 2026 meta-analysis of RCTs in infertile men found that vitamin D supplementation was associated with small but statistically significant improvements in serum testosterone alongside improvements in sperm motility (Zhang et al., 2026). A 2025 systematic review and meta-analysis of prospective RCTs in infertile men specifically looking at vitamin D3 found similar improvements in androgen levels (Jiao et al., 2025).
The consistent finding across the trial literature: men who were vitamin D-sufficient at baseline see no meaningful testosterone change from supplementation. The benefit is limited to those who start deficient. A dedicated RCT testing vitamin D in both dialysis patients and healthy subjects confirmed that testosterone levels were not significantly modified in replete participants (Ulrich et al., 2021).
What this means practically: if your 25-OH-D is below 20 ng/mL, correcting that deficiency may restore testosterone toward the normal range. If you're already at 40+ ng/mL, adding vitamin D is unlikely to move your testosterone.
Vitamin D deficiency affects 40–70% of American adults depending on geography and season. If you haven't had your levels checked, that's the first step.
Dose: Most RCTs showing testosterone effects used 3,000–5,000 IU daily for 6–12 months in deficient populations.
Zinc: Clear Effects in Deficiency, Limited Data Beyond That
Zinc is an essential mineral that directly supports testosterone synthesis. It's also a cofactor in the enzymes that regulate luteinizing hormone (LH) signaling. Severe zinc deficiency — which does happen, especially in heavy exercisers and men eating very low animal-protein diets — is clearly associated with reduced testosterone.
A systematic review examining herbs and minerals for testosterone found that zinc supplementation in deficient men consistently restored testosterone, while data in zinc-replete men was considerably weaker (Smith et al., 2021). The benefit is real, but it's a correction mechanism, not a general-purpose testosterone amplifier.
The zinc research base includes 31 studies with 8 RCTs and 3 meta-analyses — making it one of the better-studied minerals on this list (Morgado et al., 2024). Still, the honest takeaway is this: if you're not deficient, there's limited RCT evidence that extra zinc raises testosterone in otherwise healthy men.
Who benefits most: Men who train intensely and sweat heavily, those on plant-heavy diets low in red meat, and anyone not eating oysters, beef, or legumes regularly. A basic serum zinc level can tell you where you stand.
Dose used in studies: 25–45 mg elemental zinc daily. Above 40 mg long-term can interfere with copper absorption, so don't self-prescribe high-dose zinc without labs.
Magnesium: The Overlooked Mineral With Emerging RCT Data
Magnesium supports testosterone synthesis as a cofactor in hundreds of enzymatic reactions — and its evidence base (11 studies, 6 RCTs, 2 meta-analyses) is stronger than most people realize (Smith et al., 2021). Like vitamin D and zinc, the clearest effects appear in men who start deficient.
The clearest effects have appeared in men who started with low magnesium — particularly older men, athletes with high training loads, and those with metabolic syndrome. In replete men, the testosterone signal is considerably weaker.
Magnesium appears to reduce sex-hormone-binding globulin (SHBG), which increases free testosterone even if total testosterone doesn't change. Since free testosterone is the biologically active fraction, that mechanism matters.
Dose: 200–400 mg magnesium glycinate or bisglycinate daily. These forms absorb better and cause fewer GI side effects than magnesium oxide.
18.0% relative scale
increase in testosterone vs. placebo with KSM-66 ashwagandha in a randomized, double-blind, crossover trial (Lopresti et al., 2019)
Which Supplement Has the Strongest Evidence for Non-Deficient Men?
Ashwagandha (Withania somnifera, KSM-66 extract) is the supplement with the strongest RCT evidence for raising testosterone in men without a nutritional deficiency — producing 14.7–18% increases versus placebo in double-blind trials (Lopresti et al., 2019).
That trial enrolled aging, overweight males over 8 weeks — a population where the HPA-gonadal stress axis was already under pressure. A 2021 systematic review confirmed ashwagandha as the botanical with the most consistent RCT evidence across the board (Smith et al., 2021).
The mechanism runs through the hypothalamic-pituitary-adrenal (HPA) axis. Ashwagandha is an adaptogen — it lowers cortisol significantly. High cortisol suppresses testosterone production. Less cortisol means less suppression, and testosterone responds. The effect is real, but it's most pronounced in men under psychological or physical stress.
A 2023 meta-analysis of fenugreek's anabolic effects noted the same HPA-axis connection (Isenmann et al., 2023), which is why adaptogens generally show larger effects in stressed, overtrained, or sleep-deprived men than in fully rested, low-cortisol individuals.
Form and dose: KSM-66 or Sensoril at 300–600 mg daily. Generic "ashwagandha powder" products have highly variable withanolide content and weaker trial evidence.
Realistic magnitude: A 15–18% increase in a man starting at 400 ng/dL gets him to roughly 460–472 ng/dL. That's meaningful — but it won't move someone from clinically low testosterone to the mid-normal range.
Fenugreek: Positive RCTs, But Mechanisms Are Still Being Worked Out
Fenugreek (Trigonella foenum-graecum) has generated real interest because it has multiple RCTs in men showing measurable effects on testosterone. The magnitude varies, and the mechanism isn't entirely settled.
A 2024 double-blind, placebo-controlled RCT in 95 men ages 40–80 found a 12.2% increase in free testosterone index in the 1800 mg fenugreek group (Lee-Ødegård et al., 2024). A 2023 systematic review with meta-analysis found evidence of anabolic effects from fenugreek supplementation across strength and hormonal endpoints (Isenmann et al., 2023).
One proposed mechanism: fenugreek contains compounds that may inhibit 5-alpha-reductase, the enzyme that converts testosterone into DHT. By reducing that conversion, more testosterone stays in circulation. Whether this is the primary driver or whether other compounds are responsible is still being studied.
Dose used in trials: 500–600 mg standardized fenugreek extract daily. Seed-form fenugreek at lower doses has less consistent evidence.
Tongkat Ali: Promising Data, Particularly in Stressed and Aging Men
Tongkat ali (Eurycoma longifolia Jack) is a Southeast Asian herb with a growing RCT literature. A 2022 systematic review and meta-analysis of clinical trials found that Eurycoma longifolia supplementation improved serum total testosterone in men, with the effect most consistent in studies enrolling older or stressed populations (Leisegang et al., 2022).
The research base includes 17 studies with 3 RCTs and 4 meta-analyses — a smaller trial dataset than ashwagandha, but the meta-analysis level evidence is reassuring. The proposed mechanism involves stimulation of the LH-testosterone axis and, in some models, direct stimulation of Leydig cell steroidogenesis.
Tongkat ali's effects in young, healthy, low-stress men are less clear. Like ashwagandha, the signal is strongest in populations where the HPA-gonadal axis is already under pressure — aging men, men with high training loads, or men with borderline testosterone.
Dose: 200–400 mg standardized extract (standardized to eurycomanone content) daily.
Boron: Mechanistically Plausible, But the Human Trial Evidence Is Thin
Boron is a trace mineral that may raise free testosterone by suppressing sex-hormone-binding globulin (SHBG) — when SHBG falls, more testosterone circulates in its bioactive, unbound form. The current evidence base for boron's testosterone effects is limited to 9 studies with 3 RCTs and zero meta-analyses, placing it well below the evidence tier of ashwagandha or fenugreek.
The RCT data is real but modest in scale and not yet replicated widely enough to draw strong conclusions. Boron deserves continued study. It's just not on the same tier as ashwagandha, fenugreek, or tongkat ali yet.
Dose used in studies: 3–10 mg daily.
DHEA Requires Clinical Supervision — Not a Try-It-and-See Supplement
DHEA is an androgen precursor that directly raises testosterone and estradiol. Without baseline labs for DHEA-S, testosterone, and estradiol, you cannot predict how it will shift your hormone balance. In women it can cause androgenic side effects; in men it can raise estrogen alongside testosterone.
Use DHEA only under physician supervision with baseline and follow-up labs. Do not self-prescribe.
Source: Brief regulatory review; WADA Prohibited List
DHEA: An Androgen Precursor, Not a Standard Supplement
DHEA (dehydroepiandrosterone) sits in a different category from everything else on this list. It is an androgen precursor — your body converts it directly into testosterone and estradiol. The research base is substantial: 123 studies, 41 RCTs, 17 meta-analyses.
DHEA does raise androgen levels. But DHEA is not a benign "natural" supplement. It affects the entire androgen-estrogen balance. It can raise estrogen alongside testosterone, and in women it can cause androgenic side effects. It's also on the World Anti-Doping Agency (WADA) banned list for a reason.
DHEA should only be used under clinical supervision with baseline and follow-up labs. Using it without knowing your baseline DHEA-S level, testosterone, and estradiol is genuinely risky. This is not a try-it-and-see supplement.
If you suspect your DHEA-S is low (common in men and women over 40), a HEXIS provider can test your full hormone panel and determine whether DHEA makes sense as part of a supervised protocol. Schedule a consultation — we start with labs, not guesswork.
Does D-Aspartic Acid Actually Work for Testosterone?
D-aspartic acid (DAA) does not reliably raise testosterone in healthy men — despite early enthusiasm from a 2009 pilot study. Subsequent, better-designed RCTs did not replicate the finding. A meta-analysis of the full evidence base found no significant effect of DAA on testosterone in men with normal baseline levels. One short-term RCT in male climbers found only a 6.8% change that was not statistically significant (Crewther et al., 2019).
The evidence now shows that DAA does not meaningfully raise testosterone in men who aren't acutely deficient in the amino acid — which most people aren't. It remains in many supplement stacks largely because of the early study, not because the overall evidence supports it.
Tribulus Terrestris: Consistent Negative Results Across Multiple Meta-Analyses
Tribulus terrestris appears in more testosterone booster products than any other herb. It also has the most consistent negative results in rigorous research.
A 2025 systematic review of clinical trials in men found no significant testosterone effect from tribulus supplementation — the herb improved some erectile function parameters in some studies but did not increase testosterone (Vilar Neto et al., 2025). A separate 2026 meta-analysis of randomized trials on tribulus for erectile dysfunction found no testosterone signal either (Suharyani et al., 2026).
A 2014 RCT found serum testosterone values in the tribulus group ranging from 409 to 760 ng/dL across participants — not elevated relative to what you'd expect in untreated men, and without consistent separation from placebo. The 2005 RCT in young men is simply titled "The aphrodisiac herb Tribulus terrestris does not influence the androgen production in young men" (Neychev & Mitev, 2005).
Multiple independent systematic reviews, conducted years apart, all arrive at the same conclusion. Skip it.
Supplements vs. TRT: What the Numbers Actually Look Like
For a man starting at 400 ng/dL testosterone
| Best Supplement (Ashwagandha) | Testosterone Replacement Therapy | |
|---|---|---|
| Typical T increase | ~60–72 ng/dL (15–18%) | 350–550 ng/dL (2–3x) |
| Result at 400 ng/dL baseline | 460–472 ng/dL | 700–900 ng/dL |
| Evidence base | Multiple RCTs (8-12 wks) | Extensive Phase 3 trials |
| Who benefits | Low-normal T, healthy men | Clinically low T (<300 ng/dL) |
| Requires physician | No (OTC) | Yes (prescription) |
Source: Lopresti et al., 2019; Morgado et al., 2024
How Do These Supplements Compare to TRT?
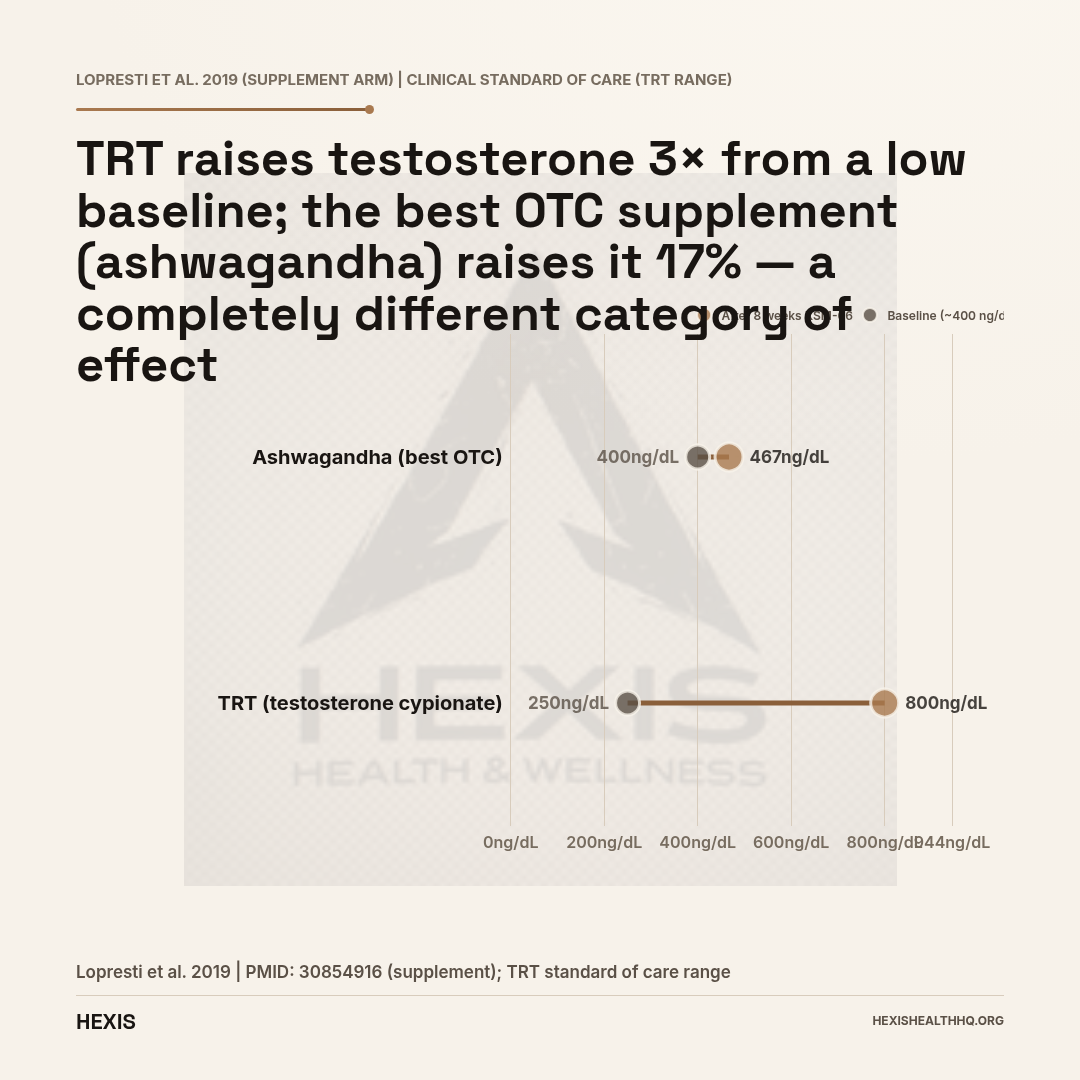
No supplement on this list comes close to TRT in magnitude — the best OTC option (ashwagandha) might raise testosterone 15–18%, while TRT typically raises it 2–3x from a low baseline.
A man starting TRT with testosterone cypionate at a standard dose will typically see his testosterone rise from, say, 250 ng/dL to 700–900 ng/dL — a 2-3x increase. Ashwagandha might raise a 400 ng/dL man to 460 ng/dL. That's a real effect, but it's not the same category.
Supplements are appropriate for:
- Men with low-normal testosterone and a documented deficiency (vitamin D, zinc, magnesium)
- Men who want to optimize their levels within the normal range before exploring TRT
- Men who have contraindications to TRT or personal reasons to avoid it
Supplements are not appropriate substitutes for TRT in men with clinically diagnosed hypogonadism. If your testosterone is below 300 ng/dL and you have symptoms, no supplement stack is going to fix that.
For a full picture of what TRT actually involves, see our HRT overview.
Does the Regulatory Status of These Supplements Matter?
Yes. These are dietary supplements regulated under DSHEA (the Dietary Supplement Health and Education Act of 1994), not drugs. Manufacturers are not required to prove efficacy before selling a product. The FDA can act after the fact if a product is unsafe, but pre-market proof of effectiveness is not required.
That matters because supplement quality varies enormously. The KSM-66 RCTs used a specific standardized extract — not the same as whatever "ashwagandha root powder" is in an unverified product at a discount retailer. If you're going to use any of these supplements, choose products with third-party testing for potency and purity. NSF Certified for Sport or USP Verified are the gold standards.
Frequently Asked Questions
Does vitamin D increase testosterone?
Vitamin D supplementation raises testosterone primarily in men who are deficient (25-OH-D below 20 ng/mL). In men who are already sufficient, RCTs generally show no significant testosterone change. Deficiency is common — get your levels checked before assuming you'll benefit.
Does zinc boost testosterone?
Zinc is essential for testosterone synthesis, and zinc deficiency is clearly associated with reduced testosterone. Supplementing corrects that deficiency and can restore testosterone to normal levels. In men who are already zinc-replete, the evidence for a further boost is much weaker.
What supplement has the best RCT evidence for testosterone in healthy men?
Ashwagandha (specifically KSM-66 extract) has the most consistent RCT evidence for raising testosterone in men who aren't nutritionally deficient. Multiple randomized, double-blind trials show 14–18% increases over 8–12 weeks versus placebo.
Does tribulus terrestris actually raise testosterone?
No. Multiple systematic reviews and meta-analyses consistently find that tribulus supplementation does not raise serum testosterone in healthy men. It may have some effects on erectile function in men with dysfunction, but testosterone is not the mechanism.
Can supplements replace TRT if my testosterone is clinically low?
No supplement will raise testosterone by the same magnitude as TRT in men with clinically low levels (below 300 ng/dL). Supplements can optimize levels within the normal range or correct deficiencies, but they are not a substitute for physician-supervised testosterone therapy when hypogonadism is the diagnosis.
What to Do With This Information
Start by getting your vitamin D, zinc, and magnesium levels actually checked — not guessed. A large fraction of men are deficient in at least one of these, and supplementing a deficiency is far more targeted than throwing ashwagandha at a problem you haven't characterized yet. If you're not sure whether your symptoms point to something hormonal, our guide to low testosterone symptoms walks through what to look for and what labs to ask about.
If your testosterone has already been measured and it's low, or if you have symptoms and want a full workup, that's a different conversation. A HEXIS provider will look at your total testosterone, free testosterone, SHBG, LH, FSH, and relevant nutrient markers — not just hand you a supplement recommendation.
Schedule a consultation if you want labs first and a protocol built around what you actually need.
Best Supplements for Testosterone: The Bottom Line
- 1
Vitamin D, zinc, and magnesium work by correcting deficiencies — if your levels are already normal, adding more won't move your testosterone. Get labs first.
- 2
Ashwagandha (KSM-66) has the strongest OTC evidence in non-deficient men: 14.7–18% testosterone increase in RCTs. Fenugreek and tongkat ali have supporting evidence. Tribulus and D-aspartic acid consistently fail in rigorous trials.
- 3
No supplement approaches TRT for men with clinically low testosterone. If your levels are below 300 ng/dL with symptoms, a physician consultation — not a supplement stack — is the right next step.