Testosterone Cypionate vs Enanthate: What the Evidence Actually Shows
Testosterone Cypionate vs Enanthate: What the Evidence Actually Shows
Testosterone cypionate and testosterone enanthate are the two most prescribed injectable testosterone formulations in the world. Most men on TRT are using one of them. And most men on TRT have wondered, at some point, whether they're on the right one.
The honest answer: for most people, it doesn't matter as much as you think. These two esters are clinically near-equivalent in practice. But the nuances are real — and understanding them helps you have a much better conversation with your provider.
The short answer: Testosterone cypionate and testosterone enanthate produce nearly identical testosterone levels at equivalent weekly doses. The only direct head-to-head trial in 234 men (Choi et al., 2022) found no statistically significant difference in trough testosterone levels. The real decision drivers are availability, cost, and injection logistics — not clinical superiority of one ester over the other.
How Do Testosterone Cypionate and Enanthate Work?
Both testosterone cypionate (TC) and testosterone enanthate (TE) are esterified forms of testosterone dissolved in an oil carrier. The ester is essentially a chemical anchor attached to the testosterone molecule — it slows the release of active testosterone from the injection site into circulation. The longer the carbon chain of the ester, the slower the release (Aboelela et al., 2026).
Testosterone cypionate has an 8-carbon ester chain (cyclopentylpropionic acid). Testosterone enanthate has a 7-carbon chain (heptanoic acid). One carbon difference. On paper, that translates to a slightly longer duration of action for cypionate. In a clinical setting with weekly injections, the difference mostly disappears.
When you inject either ester into muscle or subcutaneous fat, the testosterone-ester compound forms a depot. It releases slowly as enzymes in surrounding tissue cleave the ester linkage, freeing testosterone into the bloodstream. The kinetics of this release are what the half-life number describes.
This matters for one reason: it explains why weekly injections work for both esters, and why more frequent injections (twice weekly, every 3.5 days) smooth out the peak-to-trough swing regardless of which ester you're using.
The Half-Life Question — and Why the Numbers Are More Complicated Than They Look
Testosterone cypionate is widely quoted as having an 8-day half-life. What most sources don't say is where that number comes from: population pharmacokinetic modeling, not a classic single-dose serial-sampling study in humans. The 8-day figure is a modeled estimate, not a directly measured value from a controlled clinical PK trial. That distinction matters when someone treats it as precise biological fact.
Testosterone enanthate's half-life has been measured more directly. In non-human primates, the terminal elimination half-life for TE was 4 to 5 days after a single intramuscular injection (Weinbauer et al., 1990). A separate primate experiment found a mean half-life of 5 days (Weinbauer et al., 1990). Human data from clinical observation suggests the effective duration is closer to 7 days — consistent with why 7- to 14-day injection intervals are standard for TE.
So the range for TE is roughly 5–7 days depending on the study and the species. For TC, the modeled estimate is approximately 8 days.
The practical implication: at standard weekly injection protocols, cypionate clears slightly more slowly, which may produce marginally higher troughs heading into the next injection week. But Giagulli et al. (2011) noted that both short-acting ester formulations — TC and TE included — are characterized by their notable peak-to-trough fluctuation over the injection interval, and that smoothing those fluctuations is more a function of injection frequency than ester choice.
The difference between an 8-day and a 5–7-day half-life sounds large. In practice, when you're doing weekly injections, both esters have largely cleared and been replaced before the next dose lands. The resulting trough levels end up similar.
What the Only Direct Head-to-Head Trial Actually Found
This is where the "TC vs TE" debate either gets resolved or gets murkier depending on your definition of a winner.
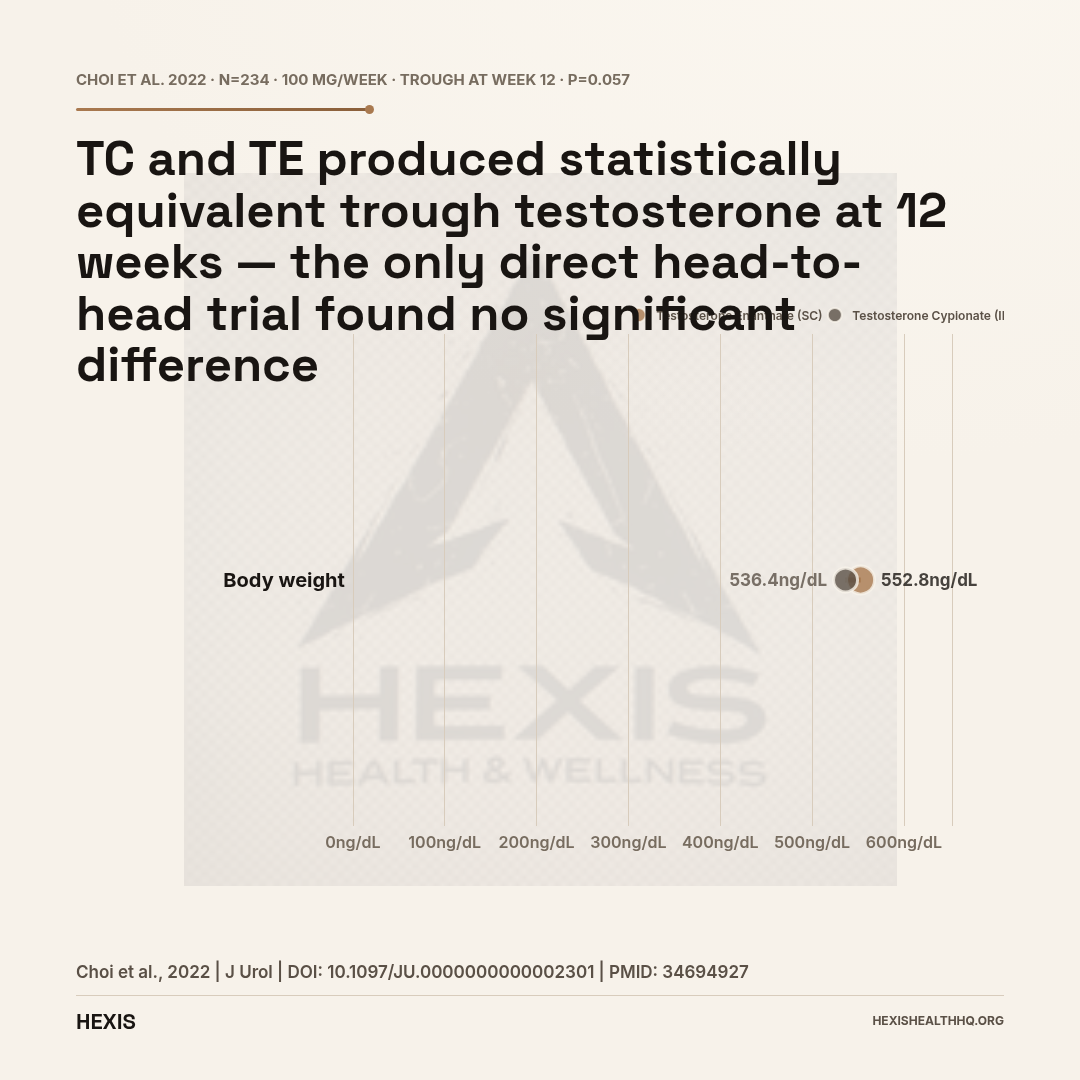
In 2022, Choi et al. published the only direct comparative trial between intramuscular testosterone cypionate and subcutaneous testosterone enanthate in hypogonadal men. The study enrolled 234 men, all treated with 100 mg weekly of either IM-TC or SC testosterone enanthate autoinjector (SCTE-AI). Testosterone levels, estradiol, hematocrit, and PSA were measured at baseline and at 12 weeks (Choi et al., 2022).
The headline result: both treatments produced significant increases in trough total testosterone from baseline. The IM-TC group went from 313.6 ng/dL to 536.4 ng/dL. The SCTE-AI group went from 246.6 ng/dL to 552.8 ng/dL. After linear regression controlling for covariates, the difference between the two groups was not statistically significant (p = 0.057) (Choi et al., 2022).
That is the most important number in this comparison. At equal weekly doses, the two esters produced statistically equivalent trough testosterone.
Where the trial did find meaningful differences: the SCTE-AI route was independently associated with lower post-therapy estradiol (p < 0.001) and lower hematocrit (p < 0.001) compared to IM-TC (Choi et al., 2022). The authors attributed this partly to the route of administration — subcutaneous delivery creates a slower, more gradual release profile with a lower peak-to-trough ratio than deep intramuscular injection — and not necessarily to the ester itself.
The Choi 2022 trial compared IM-TC against SC-TE, not IM-TC against IM-TE at the same injection site — and that matters. The differences in estradiol and hematocrit may reflect the route (IM vs. SC) as much as or more than the ester (TC vs. TE). Neither PSA nor prostate-specific outcomes differed between groups (p = 0.965) (Choi et al., 2022).
Equivalent weekly doses of TC and TE produce equivalent testosterone levels. The SC route may modestly reduce estradiol and hematocrit elevations — but that's a delivery method question, not an ester question.
Does the Route of Injection Change the Pharmacokinetics?
Yes — and this is the nuance that changes the calculation for a meaningful subset of patients.
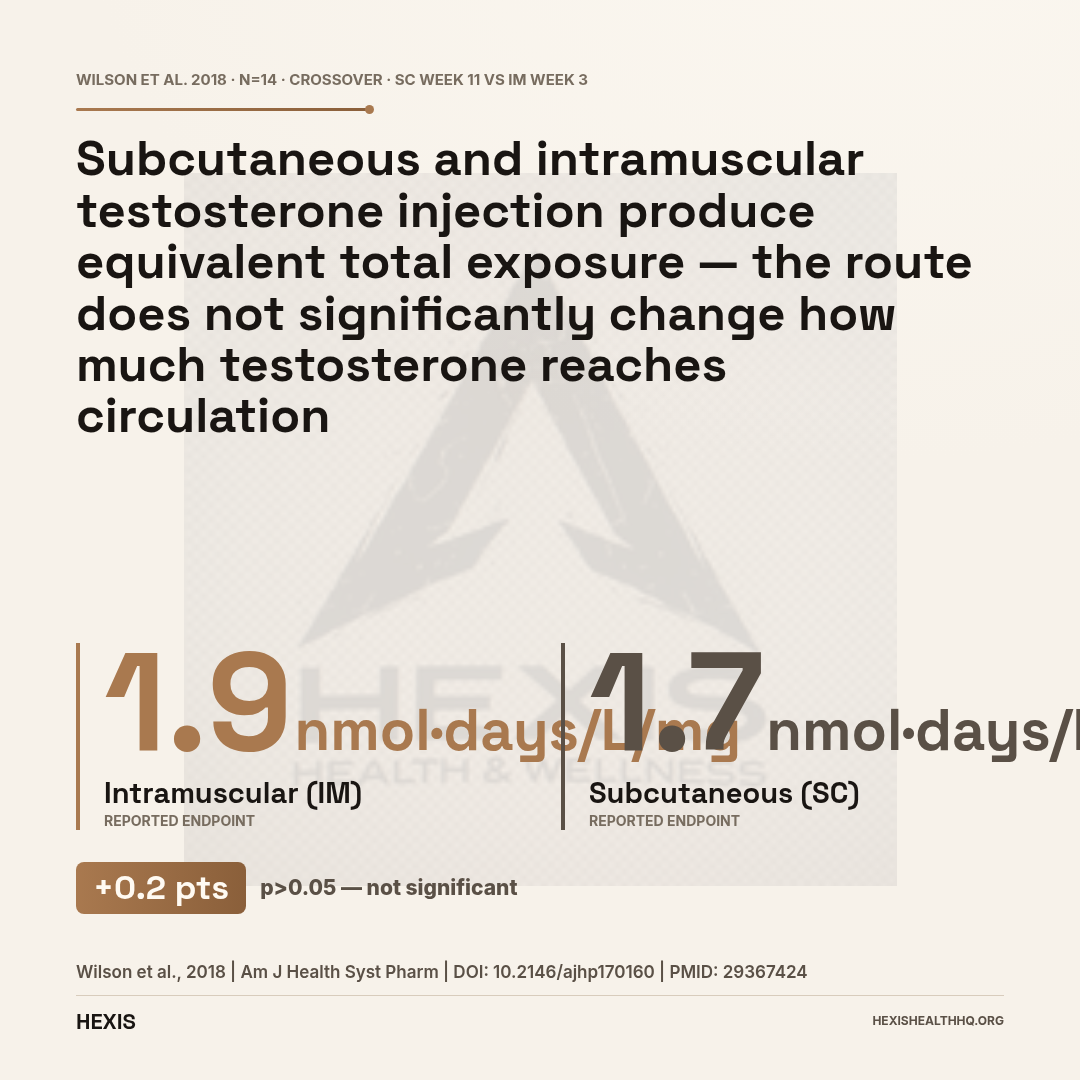
Wilson et al. (2018) compared testosterone exposure between subcutaneous and intramuscular injection in a crossover study of 14 transgender males using either testosterone cypionate or enanthate. The dose-normalized area under the concentration-time curve was 1.7 nmol·days/L/mg for SC versus 1.9 nmol·days/L/mg for IM, with no statistically significant difference (p > 0.05). Total testosterone exposure was comparable between routes (Wilson et al., 2018).
Subcutaneous injection produced equivalent testosterone exposure to intramuscular injection. Participants also reported the SC route as more tolerable — lower preinjection anxiety, less pain during injection, and less postinjection pain (Wilson et al., 2018).
Separately, McFarland et al. (2017) characterized testosterone stability in patients receiving weekly subcutaneous testosterone cypionate. Mean total testosterone across eight timepoints in a single dosing week was 627 ± 206 ng/dL, well within the normal adult male range. Free testosterone averaged 146 ± 51 pg/mL across the interval (McFarland et al., 2017). Levels were stable — not the dramatic peak-and-crash often associated with longer IM injection intervals.
Figueiredo et al. (2022) conducted a systematic review of SC testosterone administration and concluded that SC testosterone therapy at doses similar to IM results in comparable pharmacokinetics and mean serum testosterone levels. They also noted that SC is easier to self-administer and has the potential to improve patient adherence (Figueiredo et al., 2022).
If you're choosing between IM and SC delivery, the evidence says both work. SC is more comfortable and easier to self-inject consistently. The ester you use — TC or TE — matters less than whether you're actually injecting consistently at the right frequency.
The Choi 2022 trial found lower estradiol (p < 0.001) and lower hematocrit (p < 0.001) with SC-TE vs IM-TC. But this compared injection routes (IM vs SC), not just ester types. The lower estradiol and hematocrit likely reflect the blunted peak from SC delivery — not something inherent to enanthate vs cypionate.
Source: Choi et al., 2022 — J Urol, PMID 34694927
Estradiol and Hematocrit — What the Data Shows
Subcutaneous testosterone enanthate produced significantly lower estradiol and hematocrit than intramuscular testosterone cypionate at 12 weeks — but this difference reflects injection route, not ester chemistry (Choi et al., 2022).
The SCTE-AI group had significantly lower estradiol after 12 weeks compared to the IM-TC group. Hematocrit was also meaningfully lower in the SC-TE group. These are real clinical differences — elevated estradiol can contribute to fluid retention, mood changes, and gynecomastia, and elevated hematocrit raises the theoretical risk of hyperviscosity events.
But again: the comparison was IM-TC vs. SC-TE. Short-acting ester injections — whether TC or TE — produce a supraphysiological peak shortly after injection, followed by a gradual decline. That peak drives transient spikes in aromatase activity (which converts testosterone to estradiol) and in erythropoiesis (which raises hematocrit). Subcutaneous delivery blunts that peak. Giagulli et al. (2011) noted that conventional intramuscular ester injections can produce testosterone levels exceeding 2000 ng/dL within the first 24-48 hours, followed by levels dropping below 200 ng/dL near the end of the injection interval — and this extreme swing drives both estradiol and hematocrit fluctuations more than the ester chemistry does.
The practical implication: if you're managing elevated estradiol or hematocrit on IM injections, switching to SC delivery or splitting your dose to twice-weekly injections may do more good than switching from TC to TE or vice versa. Jockenhövel (2004) made this point about the limitations of conventional IM ester injections generally — the large fluctuations cause unsatisfactory shifts in mood and sexual function in some men.
Which Ester Is Easier to Get in the United States?
Testosterone cypionate is the dominant formulation in the United States. It's widely available at most retail pharmacies, often costs less, and is typically covered by more insurance plans than testosterone enanthate. Enanthate is more commonly used in Europe and other parts of the world, and is the preferred ester for many subcutaneous autoinjector formulations (including the branded SCTE-AI device studied by Choi et al., 2022).
If your clinic or pharmacy stocks one but not the other, that's your practical answer. If you're traveling internationally and need to refill a prescription, TE is more accessible outside the US.
For men managing their own injection schedule and interested in subcutaneous delivery, both esters are viable options. Wilson et al. (2018) demonstrated this directly — their crossover study included participants using both cypionate and enanthate for SC injection without protocol differences between the two.
Jockenhövel (2003) reviewed the practical limitations of conventional TE-based IM injection schedules and noted that frequency requirements and level fluctuations made this approach far from ideal for many patients. That observation applies equally to TC under the same injection schedule. The improvement most patients experience from switching to more frequent, lower-dose injections (or to SC delivery) reflects the injection logistics, not the ester.
What About Spermatogenesis and Contraceptive Use?
Both testosterone cypionate and testosterone enanthate suppress spermatogenesis at therapeutic doses — this is an expected effect of any exogenous androgen, not a property unique to either ester. Anawalt et al. (2005) confirmed this directly: TE 100 mg weekly reliably suppressed spermatogenesis to levels associated with effective male contraception in a randomized trial. Both esters suppress the hypothalamic-pituitary-gonadal axis, reducing LH and FSH and thus endogenous testosterone production and sperm output.
For any man on TRT who wants to preserve fertility options, the ester choice is less relevant than the broader conversation about sperm banking or concurrent therapies. Worth discussing with your provider before starting either.
How Do TC and TE Compare to Longer-Acting Testosterone Options?
Testosterone cypionate and enanthate are short-to-medium acting esters — distinct from long-acting testosterone undecanoate (TU), which carries a half-life of approximately 33.9 days versus the days-range half-lives of TC and TE (Behre et al., 1999). That difference means one injection every 10–14 weeks for TU versus weekly or twice-weekly for TC or TE.
The tradeoff: longer intervals are convenient, but also mean slower correction if your levels are off and a longer washout period if you stop therapy.
TC and TE sit in the middle of the spectrum — frequent enough to allow dose adjustments over weeks rather than months, long enough to support once-weekly injection protocols.
Partsch et al. (1995) compared testosterone undecanoate and testosterone enanthate head-to-head in an animal model. TE produced highly supraphysiological levels immediately after injection, with a rapid decline and lower levels in the second and third week compared to TU. The same pattern — high peak, meaningful trough — applies to TC at equivalent injection intervals. This is the fundamental pharmacokinetic trade-off of short-to-medium acting ester therapy.
Cantrill et al. (1984) described the same pattern in humans: serum testosterone rose to supraphysiological peak concentrations (mean 71 nmol/L) 24–48 hours after a mixed testosterone ester injection, followed by exponential decay to baseline after 2–3 weeks. More frequent injection intervals flatten this curve significantly.
Testosterone Cypionate vs Enanthate: Side-by-Side
The Practical Decision Framework
Neither testosterone cypionate nor testosterone enanthate is clinically superior for the average person on TRT. The best head-to-head evidence available confirms near-equivalent testosterone levels at equivalent doses. The choice in practice comes down to:
Availability: TC dominates the US market; TE is more common globally and in SC autoinjector formats.
Route: SC delivery is viable for both esters, reduces peak-to-trough swing, is better tolerated by most patients, and may marginally reduce estradiol and hematocrit elevations compared to IM. The route decision matters more than the ester decision for these parameters.
Injection frequency: Weekly or twice-weekly injections produce more stable levels than every-two-week IM injections regardless of ester choice. More frequent injection means a smoother level curve.
Your provider's preference and your insurance coverage: If your plan covers TC but not TE, start there. The clinical outcome difference is small enough that insurance and logistics should win the tiebreak.
What should not be driving the decision: internet claims that one ester is dramatically better for libido, mood, muscle gain, or estrogen management. The pharmacological basis for those claims is thin, and the only direct clinical trial doesn't support a meaningful efficacy difference.
When Should You Draw Labs on Testosterone Cypionate or Enanthate?
The half-life difference between TC and TE matters most here: when you draw labs relative to your injection day determines what number your provider sees.
Because TC clears slightly more slowly, the trough level going into injection day on a weekly protocol will be marginally higher for TC than for TE at the same dose. The difference is not large enough to change treatment decisions in most cases, but it does mean labs drawn at different points in the injection cycle will look different from each other.
Standard practice is to draw labs just before your next injection (trough). This gives you the lowest point in the cycle — the number most likely to reveal undertreatment. If your labs are drawn mid-cycle on either ester, levels will appear higher than the trough. This is a timing artifact, not a sign of a different pharmacokinetic problem (Figueiredo et al., 2022).
If you're using weekly injections of either TC or TE, draw labs on the morning of injection day, before injecting. If you're on a twice-weekly protocol, draw on whichever of the two days falls approximately 3.5 days after the previous injection.
Frequently Asked Questions
Is testosterone cypionate or enanthate better for bodybuilding?
Neither has a proven performance edge over the other. The one published direct comparison (Choi et al., 2022) found no statistically significant difference in trough testosterone at 12 weeks between TC and TE at equal doses. Both deliver testosterone; neither ester changes what the testosterone does once it's in circulation. Training, nutrition, and individual response determine outcomes — not the ester chain.
Can I switch from testosterone cypionate to enanthate?
Switching from TC to TE — or the reverse — is generally straightforward. Because the esters are near-equivalent in pharmacokinetics, the dose is usually kept the same and monitoring labs are repeated after 8–12 weeks on the new ester. Your provider should be involved in this decision and in confirming your levels after the switch.
Why does testosterone enanthate seem to cause more water retention?
There is no strong clinical evidence that TE causes meaningfully more water retention than TC at equivalent doses. Post-injection estradiol fluctuations — which can cause fluid retention — are more strongly tied to injection frequency and route than to ester type. Splitting doses to twice-weekly or switching to SC delivery tends to reduce this more effectively than switching esters (Figueiredo et al., 2022).
How often do you inject testosterone cypionate vs enanthate?
Both are typically injected weekly on modern TRT protocols. Older protocols used two-week intervals, but this creates large peak-to-trough swings in testosterone and estradiol. Weekly injections of either ester maintain more stable levels. Twice-weekly (every 3.5 days) injections produce the smoothest curves, and both esters work well on this schedule.
Does subcutaneous injection work for both testosterone cypionate and enanthate?
Yes. Wilson et al. (2018) confirmed comparable testosterone exposure between SC and IM injection using both cypionate and enanthate interchangeably in a crossover study. McFarland et al. (2017) demonstrated stable therapeutic levels across a full week using weekly SC testosterone cypionate. Both esters are viable for SC delivery with appropriate technique and needle selection.
What HEXIS Actually Does Differently
At HEXIS, we manage testosterone protocols daily. We don't pick an ester based on gut feel or habit. Your protocol starts with labs — total testosterone, free testosterone, estradiol, hematocrit, LH, FSH — and the ester, dose, and injection route are chosen based on your actual numbers and practical circumstances.
For most patients, testosterone cypionate is the starting point because of US availability and insurance coverage. Some patients do better on subcutaneous protocols — whether TC or TE — because the delivery method produces a smoother level profile and is easier to self-administer consistently. We're not attached to one option.
If you're already on a protocol and wondering whether switching esters would change anything, the honest answer in most cases is: probably not much. But if you're experiencing estradiol-related symptoms, hematocrit issues, or significant level swings, the conversation worth having is about injection frequency and route — not just ester type.
If you want a provider who will look at your full panel and give you an honest, protocol-specific answer, schedule a consultation. We start with bloodwork, not assumptions.
For more on what testosterone therapy actually looks like in practice, see our guides on understanding TRT protocols, normal testosterone levels by age, and what TRT results actually look like.
The Bottom Line on TC vs TE
- 1
At equal weekly doses, TC and TE produce equivalent trough testosterone — the only head-to-head trial (n=234) found no statistically significant difference (p = 0.057).
- 2
The half-life difference is real on paper (TC ~8 days modeled; TE ~5–7 days measured), but at weekly injection intervals the practical impact on trough levels is small.
- 3
Lower estradiol and hematocrit with SC-TE vs IM-TC in the Choi trial reflects route of delivery (IM vs SC), not the ester itself.
- 4
Choose based on availability, insurance coverage, and injection preference — not on claims of one ester being clinically superior for libido, mood, or muscle gain.
- 5
If you're managing estradiol or hematocrit issues, switch injection frequency or route before switching esters.