Does TRT Cause Infertility? Testosterone Therapy & Fertility
Does TRT Cause Infertility? Testosterone Therapy & Fertility
About 3 million American men are currently on testosterone therapy (Wenker et al., 2015). A growing number of them are in their 30s — men who still want kids, or who might want them someday. And almost none of them get a clear answer to the most important question before they start: will this make me infertile?
The honest answer: yes, TRT often impairs fertility — and in many men, it causes temporary infertility. But "temporary" is doing a lot of work in that sentence, and the nuances matter enormously.
Short answer: Exogenous testosterone shuts down your brain's signal to produce sperm. Most men see a significant drop in sperm count, and 40–70% of Caucasian men reach azoospermia (zero sperm) on standard TRT doses. Recovery is possible for most men after stopping, but timelines vary and are not guaranteed. Fertility-preserving options — including hCG, enclomiphene, and certain TRT formulations — exist and should be discussed with your provider before you ever start.
60.7% relative scale
of men on testosterone enanthate 200mg/wk reached complete azoospermia in a controlled study (Wallace et al., 1993)
How TRT Suppresses Sperm Production
Testosterone therapy suppresses sperm production by shutting down the hormonal signals the testes need to make sperm — a mechanism called HPG axis suppression that is predictable, dose-dependent, and affects most men on standard TRT doses.
Your hypothalamus releases a hormone called GnRH, which tells your pituitary to release LH and FSH. LH drives testosterone production in the testes. FSH drives spermatogenesis — the factory that produces sperm. When you introduce exogenous testosterone, your brain detects the elevated levels and shuts down GnRH output. LH and FSH crash. And without LH, intratesticular testosterone (the concentration inside your testes, which needs to be 50-100x higher than blood levels to sustain sperm production) collapses (Shiraishi et al., 2017).
This suppression is not a rare side effect — it is the predictable, mechanistic result of taking exogenous testosterone (Moss et al., 2013).
The downstream effect on sperm is significant. A controlled study using testosterone enanthate at 200mg weekly found that 17 of 28 men — 60.7% — achieved complete azoospermia (Wallace et al., 1993). Another analysis found azoospermia rates ranging from 40% to 70% in Caucasian men on testosterone-based hormonal contraceptive regimens, with rates running even higher in Asian men (Ilani et al., 2011).
That's not an edge case. For many men on TRT, the sperm factory effectively goes offline.
What Happens After You Stop TRT
Sperm production returns in most men after stopping TRT, but "most" is not "all," and the timeline is measured in months — sometimes many of them. Recovery is not guaranteed, and it is not passive.
The recovery process requires the HPG axis to restart: GnRH resumes pulsing, LH and FSH rise, intratesticular testosterone rebuilds, and the Sertoli cells — which physically support developing sperm — need time to re-engage. This sequence takes months, not weeks (McBride & Coward, 2016).
Exact median recovery times depend on the study design, duration of TRT use, baseline fertility, and age. The available evidence shows that most men who were fertile before TRT do recover spermatogenesis, but some men experience prolonged suppression requiring active treatment (Ly et al., 2005). Younger men with shorter durations of TRT use generally recover faster.
If you stop TRT specifically to conceive, plan for a recovery window of several months and work with a fertility specialist who can monitor your progress and intervene if it stalls.
Fertility-Preserving Approaches: How They Compare
For men with hypogonadism who want to maintain fertility
| hCG Co-treatment | Clomiphene / Enclomiphene | Natesto (Intranasal T) | |
|---|---|---|---|
| How it works | Mimics LH directly — maintains intratesticular T | Blocks estrogen feedback — raises endogenous LH/FSH | Short-acting T peaks may allow partial HPG activity between doses |
| Used with TRT? | Yes — added to TRT protocol | No — replaces TRT | Yes — is a TRT formulation |
| HPG axis preserved? | Partially (via direct Leydig stimulation) | Yes — fully preserved | Possibly — preliminary data only |
| Evidence quality | Established (Roth et al., 2010; Wenker et al., 2015) | Established (Earl & Kim, 2019; Rodriguez et al., 2016) | Preliminary single-center data (Ramasamy et al., 2020) |
| Best candidate | Men already on TRT who want fertility preserved | Men not yet on TRT; secondary hypogonadism | Men prioritizing fertility who need TRT |
Source: Roth et al. JCEM 2010; Earl & Kim Expert Rev Endocrinol 2019; Ramasamy et al. J Urol 2020
What Are the Fertility-Preserving Options for Men on TRT?
You don't necessarily have to choose between treating low testosterone and keeping your fertility. Several approaches can preserve or recover spermatogenesis while addressing hypogonadism.
hCG: The Most Established Co-Treatment
Human chorionic gonadotropin (hCG) mimics LH. When added to a TRT protocol, it directly stimulates Leydig cells in the testes, maintaining intratesticular testosterone even while exogenous testosterone has suppressed the natural LH signal. This preserves the hormonal environment that spermatogenesis requires (Roth et al., 2010).
Research on hCG-based recovery protocols for men who have already stopped TRT shows meaningful spermatogenesis recovery in most subjects (Wenker et al., 2015). Many reproductive endocrinologists now recommend adding hCG from the start of TRT in men who may want future fertility — rather than waiting until they want to conceive and then scrambling to recover sperm production.
For more detail on how hCG works in a TRT protocol, see our guide to hCG for men.
Clomiphene and Enclomiphene: Fertility-Preserving Alternatives to TRT
For men with hypogonadism who also want to preserve fertility, the SERM approach — using clomiphene or enclomiphene rather than exogenous testosterone — is worth serious consideration.
SERMs (selective estrogen receptor modulators) block estrogen's negative feedback at the hypothalamus and pituitary, so LH and FSH rise. That stimulates both endogenous testosterone production and spermatogenesis while keeping the HPG axis intact — sperm production is maintained, not shut down (Earl & Kim, 2019).
Enclomiphene citrate, the trans-isomer of clomiphene, has emerged as a cleaner option. It avoids some of the estrogenic effects of the clomiphene mixture while still raising LH, FSH, and endogenous testosterone in men with secondary hypogonadism (Rodriguez et al., 2016).
For men of reproductive age with secondary hypogonadism, this approach offers something TRT cannot: treating the hormone deficiency without eliminating fertility. See our full breakdown of clomiphene for men and our guide to enclomiphene for more detail.
Natesto: A TRT Formulation That May Spare the HPG Axis
Not all testosterone formulations suppress the HPG axis equally. Natesto, a short-acting intranasal testosterone delivered three times daily, produces transient testosterone peaks that clear quickly — potentially allowing the HPG axis to remain partially active between doses.
A single-center open-label trial (Ramasamy et al., 2020) reported that a substantial proportion of men maintained FSH and LH within normal range at 6 months on Natesto — a pattern distinct from the near-complete gonadotropin suppression seen with long-acting injectable or topical formulations. A separate ongoing Phase IV trial (Masterson et al., 2018) has reported similar gonadotropin-sparing observations.
These numbers are preliminary and come from small, single-center studies. They should not be treated as settled clinical fact — but the gonadotropin-sparing profile of intranasal testosterone is mechanistically plausible and continues to be studied. If preserving fertility while treating hypogonadism is a priority, Natesto is worth an informed conversation with your provider. You can read more about how it works in our Natesto guide.
Who Is Most at Risk for Prolonged Fertility Suppression?
The 60.7% azoospermia figure (Wallace et al., 1993) is sometimes misread as "most men on TRT become permanently infertile." That's not accurate — but the risk is real and should not be minimized.
Men at elevated risk for prolonged or significant suppression include:
Older men. Spermatogenesis baseline declines with age, and recovery capacity follows suit.
Men on high-dose or long-acting formulations. Injectable testosterone enanthate or cypionate at therapeutic doses produces sustained testosterone levels that maintain HPG suppression consistently. Short-acting formulations may suppress less completely.
Men with pre-existing low sperm counts. If your baseline fertility was already borderline, the margin for suppression is smaller.
Men who have been on TRT for extended periods. Duration of suppression correlates with the difficulty of recovery — though even men who have been on TRT for years can and do recover spermatogenesis with appropriate management (McBride & Coward, 2016).
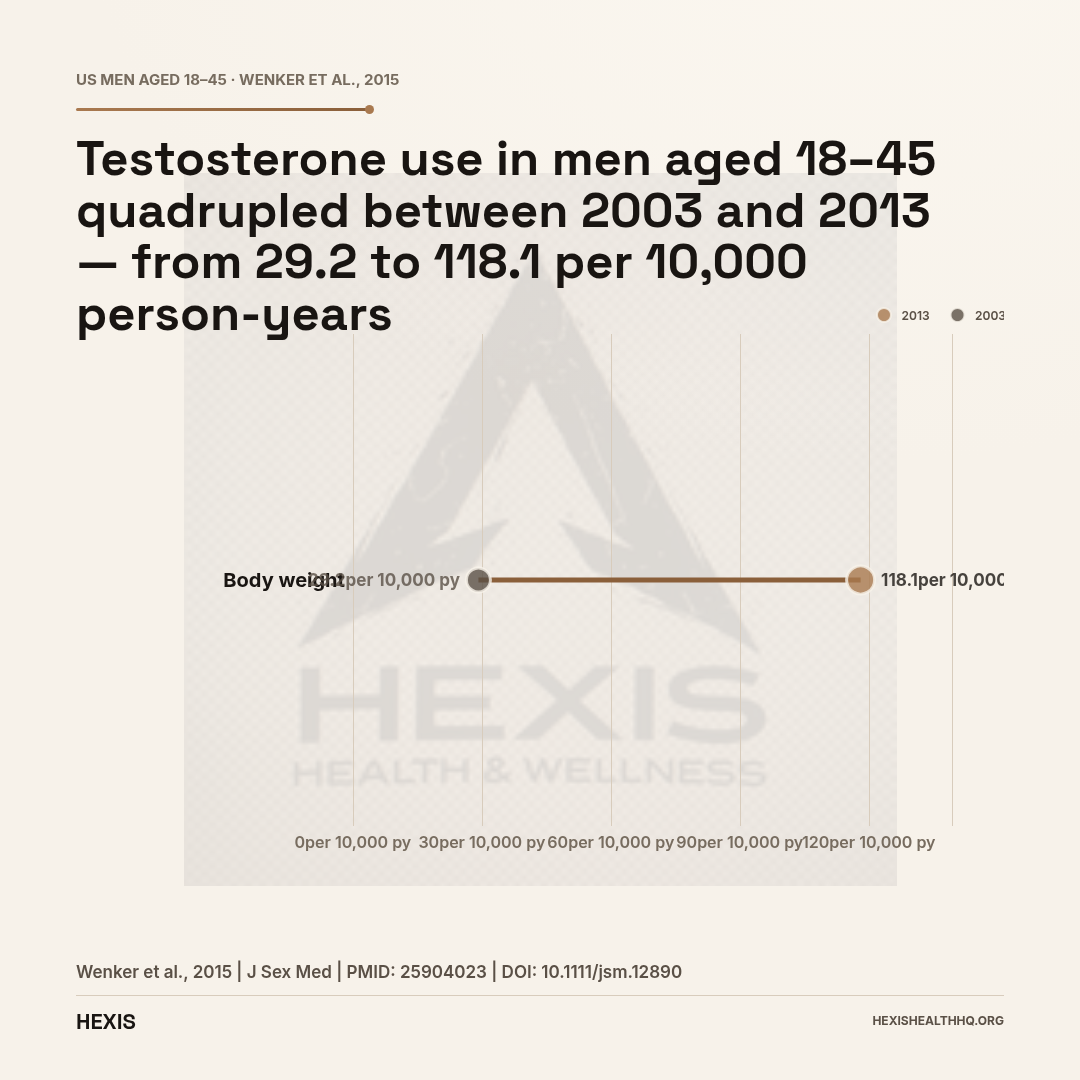
increase in testosterone use among men aged 18-45 between 2003 and 2013 — from 29.2 to 118.1 per 10,000 person-years (Wenker et al., 2015)
How Common Is TRT Use Among Men of Reproductive Age?
TRT use in men of reproductive age has grown dramatically. Between 2003 and 2013, testosterone use among men aged 18 to 45 increased more than fourfold — from 29.2 to 118.1 per 10,000 person-years (Wenker et al., 2015). The pace of that growth means a large and growing number of men are starting testosterone therapy before they have fully thought through the fertility implications.
This isn't a criticism of TRT. It's a structural counseling gap. The fertility conversation should happen before the first injection or gel application — not when a couple is trying to conceive and discovering suppressed spermatogenesis for the first time.
The evidence on managing male fertility during hypogonadism treatment has advanced considerably. A 2024 review specifically addressing reproductive-age men on TRT outlines the available interventions and supports individualized counseling based on the patient's fertility goals (Fink et al., 2024). A 2025 review similarly underscores that innovations in TRT alternatives — including gonadotropin co-therapy and SERM-based approaches — make fertility preservation realistic for most men who prioritize it (Hochu et al., 2025).
Have This Conversation Before Your First Dose
TRT can reach complete azoospermia in 40–70% of men on standard doses. Once suppression begins, recovery is not guaranteed and may require active medical intervention. Sperm banking takes one appointment and provides permanent biological insurance.
Men of reproductive age should discuss sperm cryopreservation and fertility-preserving protocols with their provider before initiating any testosterone therapy.
Source: Wenker et al., J Sex Med, 2015 (PMID 25904023)
Sperm Banking: The Belt-and-Suspenders Approach
Sperm banking before starting TRT is the single lowest-effort way to protect future fertility — one appointment, one sample cryopreserved, available indefinitely. Any man of reproductive age starting testosterone therapy should have this option explicitly offered before his first dose.
This is not pessimistic thinking — it's the same logic as buying insurance when you're healthy. Even if you plan to use hCG or another fertility-preserving strategy, having a baseline sample banked removes the "we need sperm now" pressure from any future fertility decision. If you never need it, nothing is lost. If you do, you'll be glad it's there.
Sperm cryopreservation is not a substitute for a real fertility conversation with your provider before starting TRT. But it's a low-cost insurance policy that many reproductive endocrinologists now recommend routinely for men of reproductive age starting testosterone therapy.
“The decisions made at the start of a TRT protocol are much easier to navigate than the ones made after two years of suppressed spermatogenesis.”
The Counseling Gap That's Costing Men Options
In practice, men start TRT, fertility is not discussed, sperm production drops, and by the time the issue surfaces — often when a couple is actively trying to conceive — the options are narrower and the timeline is tighter. We see this pattern documented throughout the clinical literature, and it is consistently traced back to a single failure: the fertility conversation did not happen at the start.
Providers who prescribe testosterone to men under 45 have a responsibility to address fertility explicitly. Not a line in the consent form — a real conversation about whether the patient wants children, whether hCG or an alternative approach is appropriate, and what the recovery timeline looks like if they need to stop.
The clinical tools exist — hCG co-administration, SERM alternatives, gonadotropin-sparing TRT formulations, and sperm banking. The gap is not in the options. It's in the conversation that should happen before the first prescription is written.
If your TRT provider has never asked about your fertility plans, ask them. And if you are in the process of exploring treatment for low testosterone and fertility is on your radar, bring it up at the first appointment. The decisions made at the start of a TRT protocol are much easier to navigate than the ones made after two years of suppressed spermatogenesis.
Frequently Asked Questions
Does TRT always cause infertility?
No. TRT does not cause infertility in every man, and the suppression is usually reversible. But it significantly reduces sperm production in most men — reaching complete azoospermia in 40–70% of Caucasian men on standard doses. Men who are concerned about fertility should discuss hCG co-administration, SERM alternatives, or sperm banking before starting TRT.
Can I get someone pregnant while on TRT?
Possibly, but the odds are substantially reduced. TRT suppresses sperm count significantly in most men, though it does not reliably reach zero in all cases. Azoospermia is common but not universal. Do not rely on TRT as contraception — but if you are actively trying to conceive, you should be evaluated and likely move off TRT or onto a fertility-preserving protocol.
How long does it take for sperm to come back after stopping TRT?
Recovery timelines vary considerably. Most men who were fertile before TRT do see spermatogenesis return after stopping, but the process takes months and is not immediate. Duration of prior TRT use, age, and baseline fertility all affect how long recovery takes. Men who stop TRT specifically to conceive should work with a reproductive specialist and not assume recovery is automatic.
Does hCG actually preserve fertility on TRT?
Yes, hCG is the most well-established option for maintaining intratesticular testosterone — and therefore spermatogenesis — during TRT. It works by mimicking LH, directly stimulating testicular function even when the body's own LH signal is suppressed by exogenous testosterone. It is not a guarantee, but the evidence supporting its use as a fertility-preservation co-treatment is solid (Roth et al., 2010).
Is enclomiphene better than TRT for men who want kids?
For men with secondary hypogonadism who have not yet started TRT and whose fertility is a priority, enclomiphene — or clomiphene — is often a better first choice. These medications raise endogenous testosterone by stimulating the HPG axis rather than bypassing it. The result: testosterone goes up without shutting down spermatogenesis. Not every man is a candidate, but for the right profile it avoids the fertility suppression problem at the source.
Working With a Provider on Fertility and TRT
If you're exploring testosterone therapy and fertility is on your mind — whether that's a near-term plan to have kids or a future possibility you want to keep open — the conversation with your provider needs to happen before you start, not after.
At HEXIS Health, every TRT protocol begins with a full lab panel that includes reproductive hormones. If fertility preservation is part of your goals, your provider will discuss co-treatment options including hCG, evaluate whether a SERM approach like enclomiphene fits your profile, and help you decide whether sperm banking makes sense given your timeline.
TRT and Fertility: The Bottom Line
- 1
TRT reliably suppresses sperm production — reaching complete azoospermia in 40-70% of men on standard doses. This is the mechanism, not a side effect, and it requires a real conversation before you start.
- 2
Recovery is possible for most men but takes months and is not guaranteed for everyone. Age, duration of use, and baseline fertility all affect the outcome.
- 3
Fertility-preserving options exist and work: hCG co-administration, enclomiphene or clomiphene as TRT alternatives, and Natesto's gonadotropin-sparing profile are all on the table — but only if you raise the issue before the first prescription.