Bioidentical Hormone Replacement Therapy: What the Science Actually Says
Bioidentical Hormone Replacement Therapy: What the Evidence Actually Shows
If you've spent time researching hormone options, you've almost certainly hit the word "bioidentical" — usually attached to promises that sound too good to be true. No cancer risk. Natural. Custom-made just for you. Your doctor just doesn't know about it yet.
Some of that is marketing. Some of it isn't. The actual science here is more nuanced — and more useful — than either the enthusiasts or the skeptics usually let on.
The short answer: "Bioidentical" means a hormone molecule that is structurally identical to what your own body produces. FDA-approved bioidentical hormones — estradiol patches, gels, and micronized progesterone capsules — have decades of clinical evidence behind them. Compounded bioidentical hormones, sold as personalized alternatives, carry meaningful risks that are frequently understated in marketing. The 2020 National Academies of Sciences, Engineering, and Medicine (NASEM) report found no credible evidence that compounded formulations are safer or more effective than the approved versions.
What Does "Bioidentical" Actually Mean?
The word sounds like a health claim. It isn't — it's a chemistry term.
A bioidentical hormone has the exact same molecular structure as the hormone your body produces. 17β-estradiol, the estradiol in FDA-approved patches and gels, is chemically identical to the estradiol your ovaries made before menopause. Micronized progesterone (sold as Prometrium) is identical to the progesterone your body produces. These are not copies or analogs — they are the same molecule (Kohn et al., 2019).
What "bioidentical" does NOT mean: natural, plant-derived, safe by default, or unregulated. The starting material for many bioidentical hormones is derived from wild yam or soy — but the hormone itself only exists after extensive laboratory synthesis. A wild yam contains diosgenin, which does nothing therapeutic in your body until it's chemically converted in a lab. Calling the end product "natural" is a marketing frame, not a biochemical fact.
The marketing around compounded bioidentical hormones leans heavily on "natural" as a shorthand for "safe." That logic doesn't hold up to scrutiny.
FDA-Approved Bioidentical vs. Compounded BHRT
| FDA-Approved Bioidentical | Compounded BHRT (cBHRT) | |
|---|---|---|
| FDA review | Yes — safety, efficacy, manufacturing | No — not reviewed by FDA |
| Potency standardization | Standardized batch to batch | Variable; no external verification |
| Examples | Estrace, Vivelle-Dot, Prometrium, Bijuva | Custom-mixed creams, troches, gels |
| Insurance coverage | Typically covered | Typically not covered |
| Evidence base | Full MHT clinical trial literature | No dedicated RCT database |
FDA-Approved Bioidentical Hormones: What Already Exists
You do not need to go to a compounding pharmacy to get bioidentical hormones. FDA-approved bioidentical options already exist and are widely prescribed (Soltani & Voedisch, 2026).
Estradiol (17β-estradiol) is available in multiple FDA-approved forms:
- Transdermal patches (Climara, Vivelle-Dot, Alora)
- Transdermal gels (EstroGel, Divigel)
- Transdermal spray (Evamist)
- Oral tablets (Estrace)
- Vaginal ring (Estring, Femring)
- Vaginal cream (Estrace Cream)
Micronized progesterone is available as:
- Oral capsules (Prometrium 100 mg, 200 mg)
- Vaginal gel (Crinone, Prochieve)
Estradiol + progesterone combination:
- Oral capsule (Bijuva 1 mg/100 mg)
All of these have gone through FDA review for safety, efficacy, and manufacturing quality. Their potency is standardized. The batch you get this month is the same concentration as the batch you got last month.
The main clinical argument for compounded BHRT — that you need personalized doses not available commercially — often doesn't hold up. Most women can be adequately treated with approved formulations at doses that can be adjusted over time (Stuenkel, 2021).
What Is Compounded BHRT — and What Is It Not?
Compounded bioidentical hormone therapy (cBHRT) refers to hormone preparations mixed by a 503A compounding pharmacy to fill a patient-specific prescription. These products are not FDA-approved — no compounded formulation has undergone FDA review for safety, efficacy, or manufacturing consistency. Independent testing has found real potency variability in compounded hormone products, with some containing less active ingredient than labeled and some containing more (Arnautu et al., 2025).
This doesn't mean compounded hormones are automatically harmful. It means the evidence base that would let you compare them to approved products doesn't exist. That potency variability matters when you're trying to hit a consistent hormone level.
Compounding pharmacies operate under 503A rules, which allow patient-specific prescriptions without FDA pre-approval. This is legitimate and sometimes necessary. The problem arises when compounding is marketed as a superior alternative rather than a workaround for a specific clinical need.
NASEM 2020: Compounded BHRT Claims Are Not Supported
The National Academies of Sciences, Engineering, and Medicine concluded in 2020 that there is insufficient evidence to support claims that compounded bioidentical hormones are safer or more effective than FDA-approved menopausal hormone therapy.
Source: NASEM, 2020 — The Safety and Effectiveness of Compounded Bioidentical Hormone Therapy
What the NASEM 2020 Report Actually Found
The National Academies of Sciences, Engineering, and Medicine published an independent review of compounded bioidentical hormone therapy in 2020 — probably the most thorough independent assessment of the evidence that exists.
The report's core finding: there is insufficient evidence to support claims that compounded bioidentical hormones are safer or more effective than FDA-approved menopausal hormone therapy. NASEM specifically identified 4 categories of marketing claims as unsupported by the available evidence:
Marketing claims NASEM found unsupported:
- That compounded BHRT eliminates the risk of breast cancer
- That "individualized" saliva-hormone-based dosing is scientifically validated
- That compounded formulations are better tolerated than approved products
- That the "natural" origin of bioidentical hormones confers safety advantages
Saliva hormone testing drives a significant portion of compounded BHRT prescribing — and the evidence doesn't support it. Saliva tests do not reliably reflect blood hormone levels or tissue hormone activity. The clinical validity of using saliva results to titrate hormone doses has not been established — yet it's routinely used by providers to justify highly individualized compounded protocols (Yanachkova et al., 2026).
None of this means hormone therapy in general is dangerous. It means the specific claim — that compounded hormones are meaningfully better than approved options — doesn't have the evidence behind it.
What Does the MHT Evidence Base Actually Show?
Every major clinical trial on hormone therapy — the WHI, KEEPS, the French E3N cohort — studied FDA-approved hormones, not compounded preparations. There is no separate randomized trial database for compounded BHRT. When providers cite "evidence for bioidentical hormones," they are drawing on the MHT literature, which used products like estradiol patches and micronized progesterone capsules that any pharmacy can fill. For a broader overview of that evidence, see hormone replacement therapy for menopause.
WHI 2002 and What It Got Wrong
The Women's Health Initiative trial, published in 2002, generated enormous fear about hormone therapy. But the WHI used conjugated equine estrogen (CEE) plus medroxyprogesterone acetate (MPA) — NOT estradiol plus micronized progesterone. CEE is derived from horse urine and contains multiple estrogen forms not found in the human body. MPA is a synthetic progestin with a different receptor profile than progesterone (Anagnostis et al., 2019).
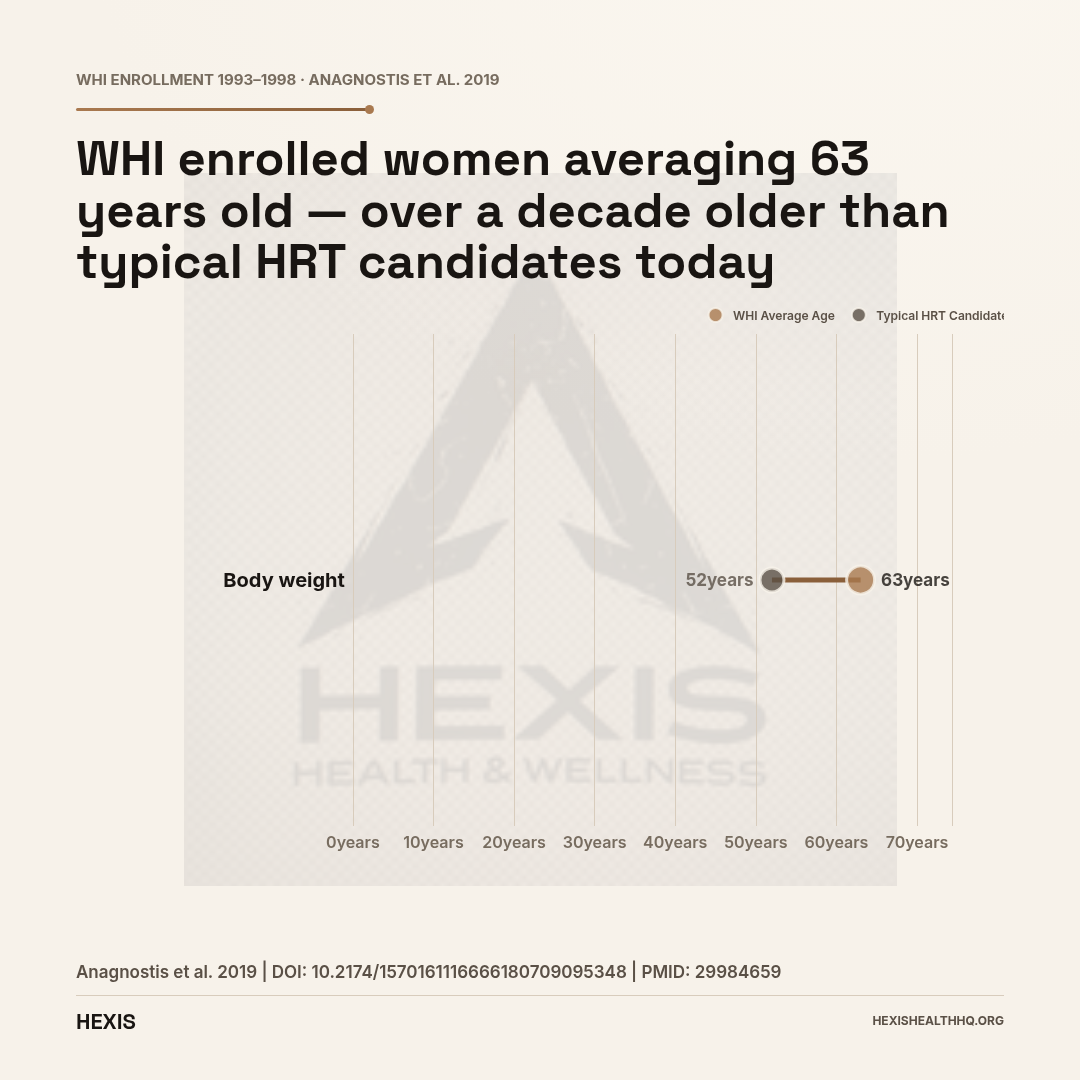
Extrapolating WHI findings to estradiol + micronized progesterone is scientifically questionable. The hormones are different. The delivery routes are different. The women enrolled were older (average age 63) and further from menopause than the women most likely to be considering HRT today.
The WHI changed prescribing patterns dramatically. Many women stopped therapy, and many physicians became reluctant to prescribe it. A significant body of subsequent research has walked back the most alarming WHI conclusions — particularly for younger women closer to menopause onset (Mauvais-Jarvis et al., 2017).
The KEEPS Trial and Transdermal Estradiol
The Kronos Early Estrogen Prevention Study (KEEPS) is one of the most informative trials for thinking about FDA-approved bioidentical estradiol. KEEPS compared low-dose transdermal 17β-estradiol, oral conjugated equine estrogen, and placebo in women who were recently menopausal (within 3 years of their last period).
Long-term follow-up from KEEPS found no significant difference in cognitive outcomes between groups — important data in the ongoing discussion of hormone therapy and dementia risk (Gleason et al., 2024). The amyloid PET and MRI analyses from the KEEPS Continuation Study showed that transdermal estradiol and oral CEE had distinct effects on brain imaging markers compared to placebo, with findings varying by APOE ε4 carrier status (Kantarci et al., 2026).
The KEEPS data is specifically useful because it used transdermal 17β-estradiol — one of the most commonly prescribed FDA-approved bioidentical options — and followed participants long enough to observe meaningful outcomes.
Route Matters: Transdermal vs. Oral Estrogen
Not all estradiol is equal in terms of risk profile. Oral estrogen undergoes first-pass metabolism in the liver, which increases clotting factor production and raises venous thromboembolism (VTE) risk. Transdermal estradiol bypasses the liver and does not produce the same clotting effect (Arnautu et al., 2025).
For women with elevated VTE risk, transdermal estradiol is generally preferred. For most women without specific contraindications, the cardiovascular risk profile of transdermal estradiol combined with micronized progesterone appears more favorable than the combination studied in the WHI (Anagnostis et al., 2019).
Progestogen Type Matters Too
The breast cancer signal in the WHI was largely driven by the progestin arm (CEE + MPA). Micronized progesterone has a different receptor profile and a different observed risk pattern. The French E3N cohort study — one of the largest observational studies on this question — found that estrogen combined with micronized progesterone was associated with a lower breast cancer risk than estrogen combined with synthetic progestins (L'Hermite, 2017).
Micronized progesterone is not risk-free. But the risk profile appears different from synthetic progestins, and using WHI breast cancer data to counsel women on estradiol + micronized progesterone regimens overstates the actual risk.
What Hormone Therapy Can Actually Do
FDA-approved menopausal hormone therapy reliably treats vasomotor symptoms, protects bone density, and addresses genitourinary syndrome of menopause — and that evidence comes from multiple independent clinical trials, not one disputed study. It is supported by the major professional societies including the Menopause Society (NAMS) and the International Menopause Society.
Hot Flashes, Night Sweats, and Vaginal Symptoms
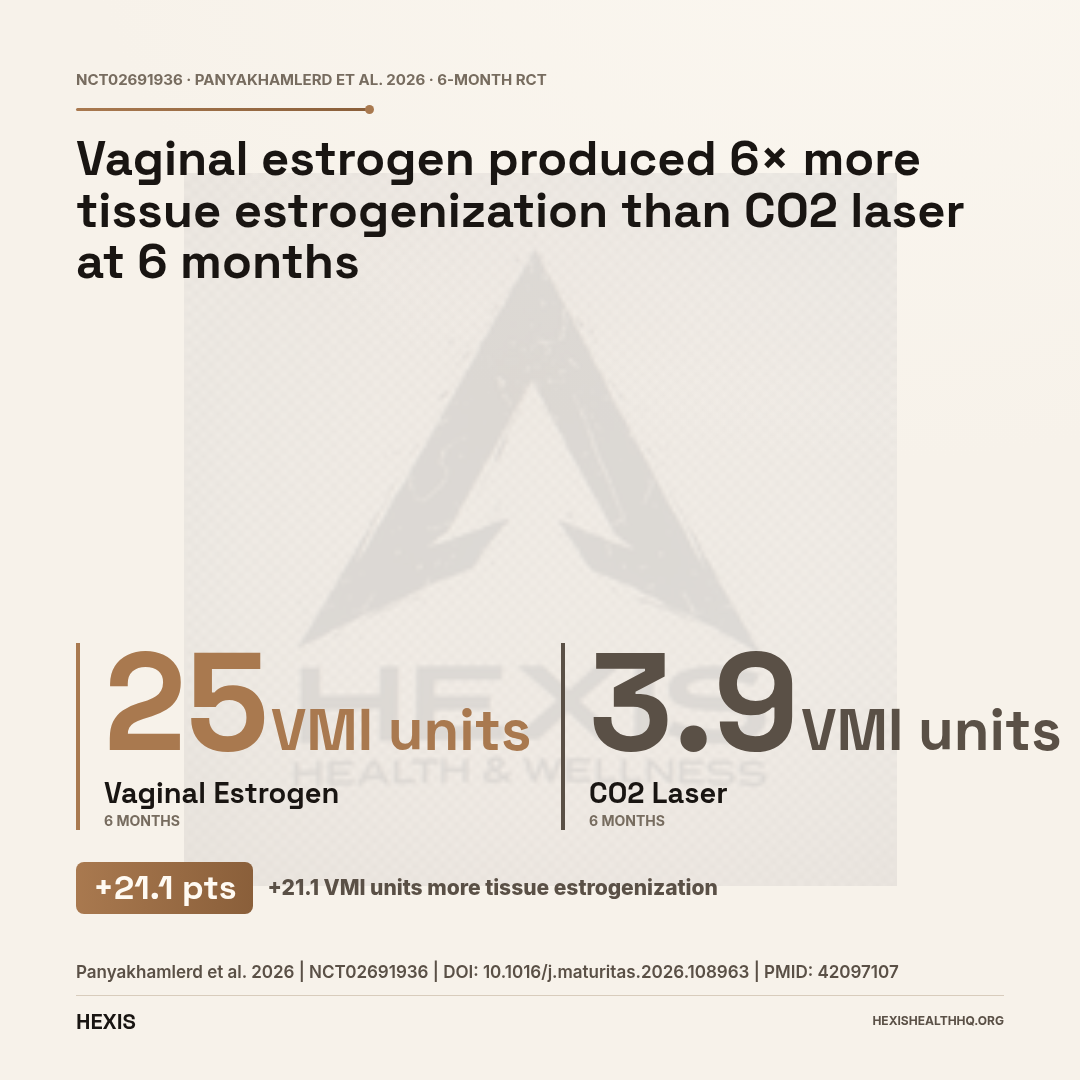
Hot flashes and night sweats are the primary symptom indication. FDA-approved estradiol formulations are among the most effective treatments available for vasomotor symptoms. Local vaginal estrogen therapy also reliably addresses genitourinary syndrome of menopause — vaginal dryness, discomfort with intercourse, urinary symptoms. A randomized placebo-controlled trial comparing vaginal estrogen therapy to laser therapy found vaginal estrogen produced meaningful improvements in vaginal dryness scores (−5.76 units vs. laser at −5.48 units at 6 months) and superior effects on vaginal maturation index (25 units vs. 3.9 units at 6 months) (Panyakhamlerd et al., 2026).
Bone Protection
Menopausal hormone therapy preserves bone mineral density and reduces fracture risk in postmenopausal women. The evidence here is among the strongest in the MHT literature — this is one of the indications where the benefit-risk calculation is most clearly favorable for women at risk of osteoporosis (Gosset et al., 2021; Rozenberg et al., 2020). For the full picture on estradiol delivery options, see estradiol patch guide.
Brain Fog, Mood, and Cognition
The relationship between hormone therapy and cognition is an active research area. Perimenopausal hormone fluctuations are associated with mood symptoms, cognitive complaints, and sleep disruption. HRT addresses these symptoms for many women through hormonal stabilization (Langhe et al., 2026). Long-term cognitive effects remain under study, with the KEEPS Continuation findings suggesting no harm to cognition from estradiol-based therapies in recently menopausal women (Gleason et al., 2024).
Joints and Musculoskeletal Pain
MHT shows benefits for musculoskeletal symptoms in perimenopause. A 2025 trial found menopausal hormone therapy superior to complementary medicine for symptomatic hand osteoarthritis in perimenopausal women (Sasaki et al., 2025). A randomized factorial trial also found MHT plus exercise improved outcomes in women with greater trochanteric pain syndrome (McMillan et al., 2022).
“Individualization is not the same as efficacy. A dose can be individualized based on symptoms, labs, and clinical response using approved products with known potency.”
Marketing Claims vs. Evidence: The Honest Breakdown
Four claims dominate compounded BHRT marketing. None of them hold up to scrutiny when checked against the clinical literature.
"Bioidentical hormones have no cancer risk." False. All hormone therapy carries risks that must be weighed against benefits. Estrogen alone in a woman with an intact uterus increases endometrial cancer risk without a progestogen. The breast cancer signal varies by regimen and duration. FDA-approved bioidentical formulations are not exempt from these considerations — their advantage is a more favorable risk profile compared to CEE + MPA, not zero risk (Thorat et al., 2026).
"Saliva testing gives a personalized hormone profile." Not supported. Saliva hormone levels are highly variable, not validated as a measure of systemic hormone status, and do not reliably predict clinical need. Using saliva results to drive prescribing decisions is a practice that lacks a solid evidence foundation (Yanachkova et al., 2026).
"Compounded hormones are more natural." The "natural" framing is marketing language. The synthesis process for compounded bioidentical hormones is identical to that used for FDA-approved versions — the difference is the regulatory oversight applied after synthesis, not the origin of the molecules.
"Compounded BHRT is individualized, so it must be better." Individualization is not the same as efficacy. A dose can be individualized based on symptoms, labs, and clinical response using approved products with known potency. The argument that compounded pharmacies provide superior personalization has not been tested in controlled trials against approved alternatives.
Who Actually Needs Compounded Hormone Therapy?
Compounded hormone therapy is clinically appropriate for a narrow set of patients: those with documented allergies to inactive ingredients in approved products (such as peanut oil in some Prometrium formulations) and those who require a specific dose or delivery route not commercially available. For most women seeking hormone therapy, these conditions do not apply.
The concern isn't that compounding should be banned. It's that compounding is frequently marketed as the preferred option for everyone rather than a clinical workaround for a specific need. When that happens, patients are paying more (compounded products typically aren't covered by insurance), getting less quality assurance, and sometimes using hormone testing methods that aren't clinically validated — without a meaningful benefit over what's already available and approved (Stuenkel, 2021).
If you are considering hormone therapy, starting with FDA-approved options makes sense. If you have a specific clinical need that approved formulations can't meet, compounding becomes a reasonable conversation to have with your provider. Understanding the full hormone replacement therapy evidence base is a good starting point before that conversation.
Frequently Asked Questions
Is compounded BHRT FDA-approved?
No. Compounded bioidentical hormone preparations are made by 503A pharmacies and are not FDA-approved for safety, efficacy, or manufacturing quality. The 2020 NASEM report found insufficient evidence that compounded BHRT is safer or more effective than FDA-approved menopausal hormone therapy. FDA-approved bioidentical options — estradiol patches, gels, and micronized progesterone capsules — already exist and have extensive clinical data behind them.
Are bioidentical hormones safer than synthetic HRT?
The word "safer" requires context. FDA-approved bioidentical formulations — transdermal estradiol plus micronized progesterone — appear to have a more favorable risk profile than the CEE plus medroxyprogesterone acetate combination studied in the Women's Health Initiative. But "bioidentical" does not mean risk-free, and compounded bioidentical products lack the standardized potency and quality oversight of approved options.
What is the difference between Prometrium and compounded progesterone cream?
Prometrium is FDA-approved oral micronized progesterone with standardized potency, quality-controlled manufacturing, and a substantial clinical evidence base. Compounded progesterone cream is a custom preparation with variable potency, no FDA oversight, and limited evidence that it produces adequate systemic progesterone levels to protect the uterine lining — a critical consideration in women with an intact uterus using systemic estrogen.
What did the NASEM 2020 report conclude about compounded bioidentical hormones?
The National Academies of Sciences, Engineering, and Medicine 2020 report concluded that there is insufficient evidence to support claims that compounded bioidentical hormones are safer or more effective than FDA-approved menopausal hormone therapy. The report specifically called out as unsupported: claims of eliminated cancer risk, the use of saliva testing to drive hormone dosing, and the broader marketing framework around compounded BHRT.
Is transdermal estradiol different from oral estrogen in terms of blood clot risk?
Yes — meaningfully so. Oral estrogen undergoes first-pass liver metabolism, which increases clotting factor production and raises venous thromboembolism (VTE) risk. Transdermal estradiol bypasses the liver, does not produce the same clotting effect, and is generally preferred for women with elevated cardiovascular risk. This is one reason FDA-approved transdermal formulations are often the first choice for estrogen delivery in clinical practice.
Working with a Provider Who Actually Reads the Evidence
Hormone therapy decisions require real lab work, a full symptom history, and an understanding of your personal risk factors — not a saliva test and a custom-compounded cream based on marketing claims. At HEXIS, we see patients who have been told they need compounded hormones based on saliva testing, when the same clinical goal — stable, evidence-based hormone levels — could be reached with an FDA-approved patch or capsule covered by insurance.
HEXIS providers start with bloodwork. The protocol follows from what your labs and symptoms actually show, not from a default formula. If FDA-approved options cover your clinical needs, that's what gets prescribed — with the quality assurance and evidence base those products carry. If there's a specific reason compounding makes clinical sense for you, that conversation happens with your eyes open.
Schedule a consultation to talk through your hormone health with a provider who works from current evidence, not wellness industry sales copy.
- 1
"Bioidentical" is a chemistry term, not a safety claim — it means the molecule matches what your body makes.
- 2
FDA-approved bioidentical hormones already exist: estradiol patches, gels, sprays, and micronized progesterone (Prometrium) are all bioidentical and fully reviewed.
- 3
Compounded BHRT is not FDA-approved and lacks standardized potency — the 2020 NASEM report found no evidence it is safer or more effective.
- 4
The MHT evidence base (WHI, KEEPS, E3N cohort) used FDA-approved hormones. Transdermal estradiol + micronized progesterone has a more favorable risk profile than CEE + MPA.
- 5
Saliva hormone testing is not a validated way to drive dosing decisions.
- 6
Start with approved options. Compounding is a workaround for a specific clinical need, not the default.