Clomid for Men: How It Works, What It Does to Testosterone, and Why Fertility Changes Everything
Clomid for Men: How It Works, What It Does to Testosterone, and Why Fertility Changes Everything
Most men who look into low testosterone assume there are two choices: testosterone replacement therapy (TRT) or nothing. There is a third option — one that raises your body's own testosterone production while keeping your sperm count intact. That option is Clomid for men, and it's been used off-label in urology and men's health clinics for decades.
Quick answer: Clomid (clomiphene citrate) is a SERM — a selective estrogen receptor modulator — that blocks estrogen receptors in the hypothalamus. This removes a key brake on the hormonal system, causing the pituitary to release more LH and FSH, which in turn drives the testes to produce more testosterone and support sperm production. Clinical trials show average testosterone increases of 273 ng/dL or more, while preserving fertility — the core reason men choose it over TRT.
What Is Clomid and Why Is It Used Off-Label in Men?
Most people know Clomid as a female fertility drug. It was FDA-approved in 1967 for ovulation induction in women with certain ovulatory disorders — and that is still its only official indication. Its use in men with hypogonadism or infertility is entirely off-label.
That off-label status doesn't mean it's fringe medicine. It means the formal approval process, which is expensive and drug-company-driven, never happened for men. The clinical data exists. Physicians at academic medical centers and urology practices have been prescribing it for men for over 30 years (Wheeler et al., 2019).
The active ingredient is clomiphene citrate. Under the hood, it is actually a mixture of two isomers — more on that later, because it matters for side effects.
How Clomid Works in Men: The Hypothalamus Is the Key
To understand how Clomid raises testosterone, you need a 30-second refresher on what normally keeps testosterone levels in check.
Your brain — specifically the hypothalamus — monitors circulating estrogen and testosterone through negative feedback. When levels are adequate, the hypothalamus dials back its signal (GnRH), the pituitary releases less LH and FSH, and the testes produce less testosterone as a result. The system self-regulates.
Clomid blocks estrogen receptors in the hypothalamus. The brain can no longer detect estrogen clearly, so it perceives a deficit and responds by releasing more GnRH. The pituitary responds with more LH (which tells the Leydig cells in the testes to make testosterone) and more FSH (which drives spermatogenesis in the Sertoli cells). Testosterone rises — but crucially, it rises through your own testes (Herzog et al., 2020).
This is exactly what does NOT happen on TRT. When you inject or apply exogenous testosterone, the hypothalamus detects plenty of hormone and shuts down LH and FSH almost completely. Intratesticular testosterone drops, sperm production craters, and many men on TRT eventually develop azoospermia. If you want to father children while treating low T, Clomid works through a fundamentally different pathway.
That mechanism — raising testosterone while preserving the HPG axis — is the entire clinical case for using Clomid in men who want to keep their fertility options open. For more on how TRT affects sperm production, see our article on TRT and fertility.
Who Is a Candidate for Clomid?
Clomid works for men with secondary (hypogonadotropic) hypogonadism — low testosterone caused by insufficient brain signaling, not by failed testes. It does not work for primary testicular failure. That distinction — intact HPG chain versus damaged testes — is the first thing any physician should confirm before prescribing it.
Secondary (hypogonadotropic) hypogonadism is the target. Labs typically show low T alongside low or low-normal LH and FSH — the testes are capable of producing testosterone, they are just not getting the signal to do so. Clomid restores that signal.
Primary hypogonadism is a different situation. If the testes themselves are damaged or absent (from Klinefelter syndrome, orchidectomy, or radiation damage), there is nothing downstream to stimulate. Clomid will not work in that setting.
The other common use case: men on TRT who want to recover fertility. Because TRT suppresses LH and FSH to near-zero, sperm production stops. Transitioning off TRT and onto Clomid is one pathway back to spermatogenesis — and some physicians use HCG in combination. If you are exploring that transition, the details are in our HCG for men article.
ng/dL mean testosterone increase across SERM vs placebo RCTs — 95% CI: 191.87–355.66 (Hohl et al., 2025)
What Does the Evidence Actually Show?
The clinical evidence for Clomid in men is consistent: testosterone rises meaningfully, LH and FSH activate alongside it, and sperm parameters improve in most men. The data is not perfect — most of it is retrospective, and there are no large randomized trials comparing it head-to-head against TRT for all outcomes — but across 19+ studies and over 1,200 men, the signal holds.
Testosterone Increases
A 2025 systematic review and meta-analysis of randomized controlled trials comparing SERMs (clomiphene and enclomiphene) to placebo found a mean difference in total testosterone of +273.76 ng/dL (95% CI: 191.87–355.66) (Hohl et al., 2025). That is a clinically meaningful increase — enough to move most hypogonadal men from the low zone into the normal range.
A 2022 systematic review and meta-analysis looking specifically at clomiphene citrate for hypogonadism across 19 studies and 1,279 men found testosterone increased by 2.60 nmol/L (95% CI: 1.82–3.38) (Huijben et al., 2022).
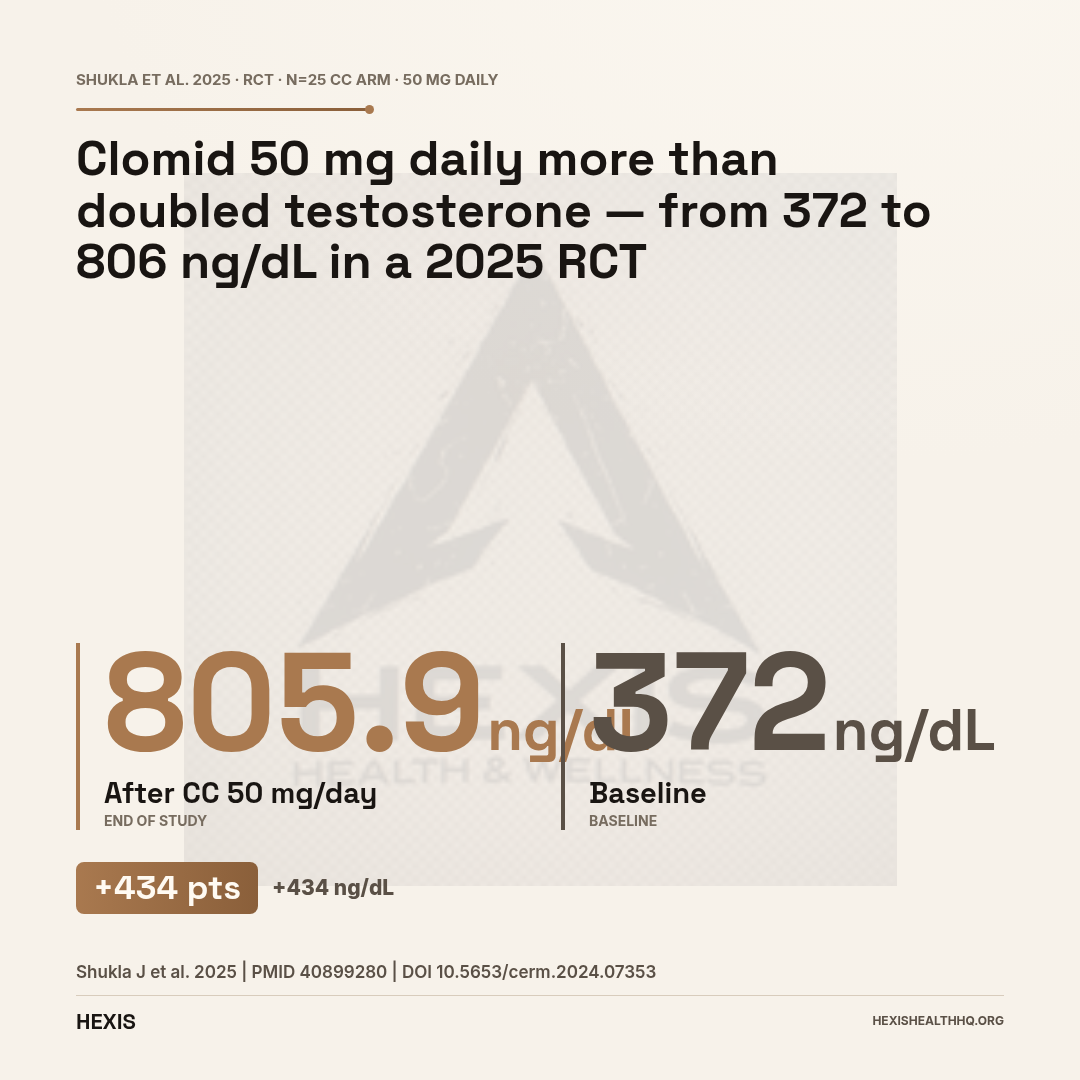
In a more recent randomized controlled trial with 50 men with oligoasthenozoospermia given 50 mg CC daily, mean testosterone rose from 371.97 to 805.94 ng/dL — more than doubling from baseline (Shukla et al., 2025). That is a dramatic individual-level result.
The typical clinical range you will see in practice is a rise of 150–300 ng/dL in population averages, with some men responding much more aggressively.
LH and FSH Rise in Parallel
Clomid works by increasing pituitary signaling, so LH and FSH rise alongside testosterone — that's the whole mechanism at work. In one prospective cohort, LH increased by +4.8 IU/L and FSH by +4.9 IU/L after Clomid treatment (Roque et al., 2026). The brain-pituitary-testis axis is activating, not being bypassed.
Clomid Can Reduce Sperm Count in Some Men
A 2021 systematic review found that between 19% and 24% of men treated with clomiphene citrate experience a counterintuitive drop in sperm count, concentration, motility, or total motile sperm — not an improvement. Of those who stopped treatment due to the decline, up to 17% did not recover to their baseline values.
Baseline and follow-up semen analysis is not optional if fertility is your goal. Discuss monitoring frequency with your physician before starting.
Source: Gundewar et al., Andrologia, 2021
Does Clomid Improve Sperm Quality?
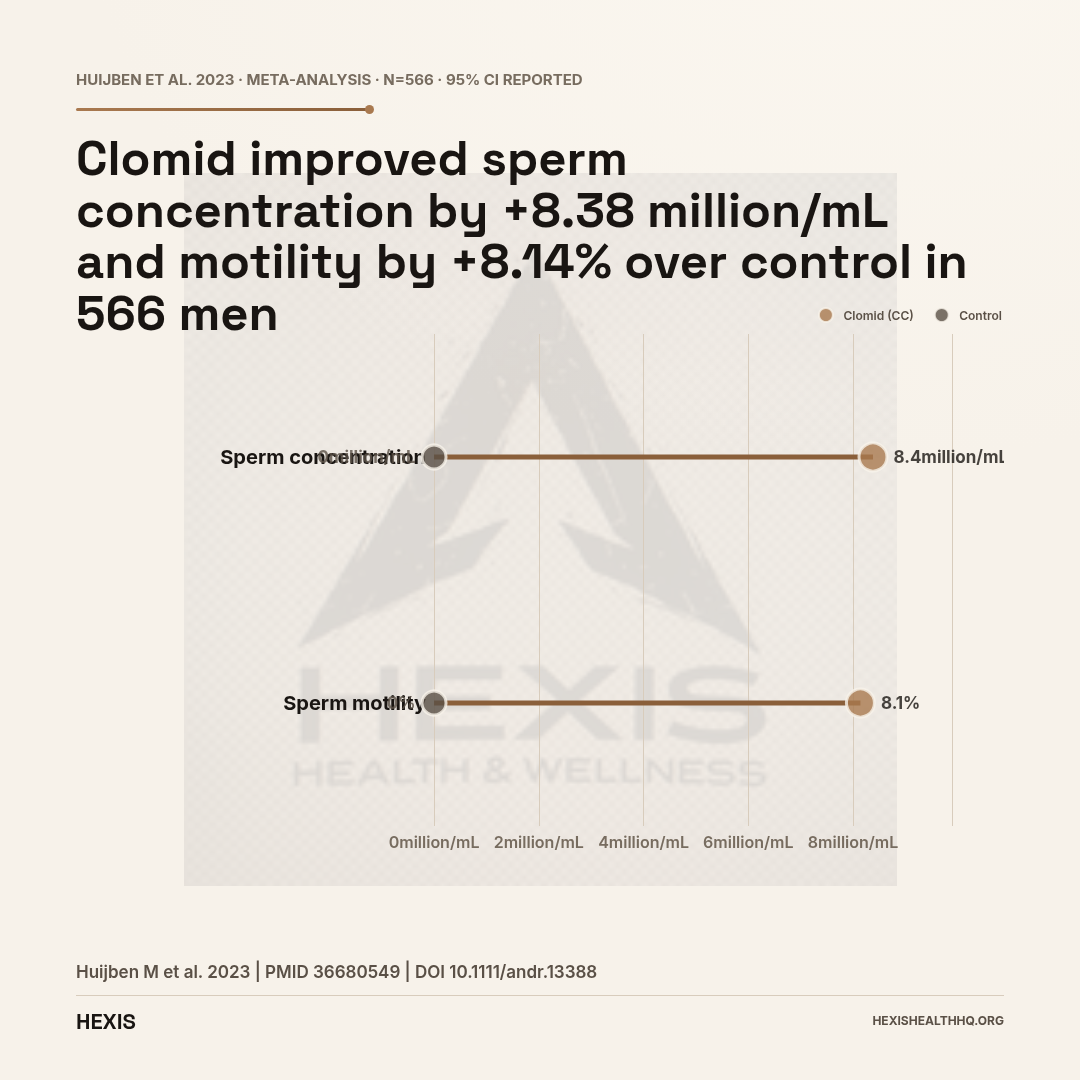
Clomid improves sperm concentration and motility in most men — a 2023 meta-analysis of 566 men found a mean increase of +8.38 million/mL in sperm concentration and +8.14% in total motility (Huijben et al., 2023). However, between 19% and 24% of men experience a paradoxical decline instead. This counterintuitive risk is documented and warrants monitoring before and during treatment.
The Positive Data
Pregnancy rates in the included studies of that 2023 meta-analysis ranged from 0 to 40%, averaging around 17% (Huijben et al., 2023) — a wide range that reflects how variable male infertility etiology is across study populations.
In the 2025 RCT cited above, sperm concentration rose from 9.17 to 13.88 million/mL alongside the testosterone increase (Shukla et al., 2025).
A 2025 network meta-analysis comparing multiple pharmacological approaches to idiopathic male infertility found that CC 25 mg every other day ranked first for improving sperm concentration (MD = 22.00; 95% CI: 14.75–29.25; P-score = 99%) out of all non-hormonal and hormonal treatment arms studied (Santi et al., 2025).
For men with low sperm counts who want to improve their fertility numbers without resorting to TRT, that is a strong evidence base.
The Paradoxical Decline — A Real Signal, Not a Footnote
A 2021 systematic review confirmed the paradoxical decline signal with specificity: sperm count, concentration, motility, and total motile sperm count all declined in affected men — not one parameter but all four (Gundewar et al., 2021). Of those who stopped treatment due to the decline, up to 17% did not recover to their baseline.
Nobody knows reliably who will respond this way. The leading theory involves estrogen excess — high E2 impairing spermatogenesis at the testicular level — but individual variability in receptor sensitivity plays a role too. What it means practically: semen analysis before and during treatment is not optional. If your sperm count drops on Clomid, you and your physician need to know quickly.
This is not a reason to avoid Clomid — the majority of men benefit. But burying this number in a footnote would be dishonest.
For a fuller discussion of male fertility treatment strategies, see our article on enclomiphene, which covers the purified active isomer.
Clomid vs. Testosterone Replacement Therapy
Key clinical differences for men considering treatment
| Clomid (CC) | TRT (Injections/Gels) | |
|---|---|---|
| Testosterone source | Endogenous (your own testes) | Exogenous (external) |
| Fertility preserved? | Yes — LH/FSH maintained | No — HPG axis suppressed |
| Sperm production | Maintained or improved* | Suppressed (>60% azoospermia) |
| Polycythemia risk | 1.07–1.7% | 2.22–11.2% |
| Testosterone predictability | Variable — depends on HPG axis | High — dose-controlled |
| FDA approval (men) | Off-label | Approved (hypogonadism) |
| Best candidate | Secondary hypogonadism + fertility goals | Primary or secondary hypogonadism, no fertility concern |
Source: Wheeler et al. 2016; Tadisina et al. 2026; Gundewar et al. 2021 (*paradoxical decline in 19–24%)
Clomid vs. TRT: The Comparison That Actually Matters
The choice between Clomid and TRT is not a question of which raises testosterone more. TRT typically delivers higher and more predictable T levels. The question is what else you are trading away.
The Fertility Tradeoff
TRT suppresses LH and FSH to near-zero. This means the testes stop producing sperm. Studies on male hormonal contraception show azoospermia rates over 60% in men on adequate TRT doses. Recovery after stopping is not guaranteed, and it can take 12–24 months. If you plan to have children, this is the central issue.
Clomid preserves the HPG axis. Sperm counts can improve, stay stable, or — in the minority of cases above — paradoxically decline. But you are not deliberately switching off the factory.
The Safety Comparison
A large retrospective study of US Veterans (n = 2,518 matched patients) compared Clomid to TRT across several adverse outcomes (Tadisina et al., 2026). Key findings:
- Polycythemia: 1.07% (CC) vs. 2.22% (TRT)
- New-onset hypertension: 6.04% (CC) vs. 10.48% (TRT)
- All-cause mortality: 1.83% (CC) vs. 10.13% (TRT)
The mortality difference is striking, but this study has major methodological limitations. It was retrospective and non-randomized. The TRT group was substantially older than the CC group — and age is the most powerful predictor of mortality. This is not a clean apples-to-apples comparison. The polycythemia and hypertension differences are more likely to reflect a real pharmacological advantage of CC, since those outcomes are known mechanistic effects of exogenous testosterone (Wheeler et al., 2016).
For context, a multi-institutional study found polycythemia in 1.7% of CC users versus 11.2% of TRT users (p = 0.0003), while testosterone increases were similar between groups — 367.6 ng/dL (CC) vs. 333.1 ng/dL (TRT) (Wheeler et al., 2016).
The practical takeaway: for men who want normal testosterone without the erythrocytosis risk of TRT, and especially for men who want to preserve fertility, Clomid offers a real mechanistic advantage.
“Clomid is not a pure compound. It is a non-racemic mixture of two structural isomers — enclomiphene, the anti-estrogenic isomer that drives testosterone up, and zuclomiphene, which accumulates over time and may work against it.”
The Isomer Problem: Why Long-Term Clomid Has a Wrinkle
Clomiphene citrate (Clomid) is not a single molecule — it is a non-racemic mixture of two structural isomers with opposite hormonal effects: enclomiphene (~62%), which is anti-estrogenic and drives the testosterone increase, and zuclomiphene (~38%), which has weak estrogen-agonist activity and accumulates in the body over time (Helo et al., 2017). This distinction matters for long-term safety.
- Enclomiphene (trans-clomiphene, ~62%): Blocks hypothalamic estrogen receptors and drives the LH/FSH rise — the active, therapeutic isomer.
- Zuclomiphene (cis-clomiphene, ~38%): Weak estrogen-agonist activity with a much longer half-life, leading to progressive accumulation with continued dosing.
The clinical concern: as zuclomiphene builds up, it may partially counteract enclomiphene's anti-estrogenic effect, or directly contribute to estrogenic side effects — mood changes and elevated E2 are the most reported (Helo et al., 2017).
This is why enclomiphene — the purified trans-isomer sold as Androxal — was developed separately. It delivers the therapeutic effect without the zuclomiphene burden. If you want to dig into how they compare, the enclomiphene article covers the isomer-specific trial data.
For most men on shorter-term CC protocols (months, not years), the zuclomiphene accumulation concern is lower. For long-term users, it is worth discussing with your physician.
What Are the Side Effects of Clomid in Men?
Clomid's side effect profile is generally milder than TRT's — no polycythemia risk, no injection site reactions, no testicular atrophy. But three specific risks require attention: mood changes (the most reported), visual disturbances (the most serious), and paradoxical sperm decline (the most counterintuitive). Each is documented in peer-reviewed literature and each warrants monitoring.
Mood and Emotional Changes
Men in practice report mood-related effects more than any other side effect — though it's the least well-studied in the male literature. Zuclomiphene's estrogenic activity, combined with fluctuating T and E2 during titration, can produce irritability, mood swings, and in some cases depressive symptoms. These tend to be dose- and duration-dependent.
Visual Disturbances
Stop the medication and call your doctor the same day if your vision changes on Clomid. That is not an overreaction — it is the appropriate response. A review found documented cases of blurred vision, palinopsia (trailing of visual images), scotomata (blind spots), and in rare cases central retinal vein occlusion (Viola et al., 2011). Separate case reports have documented palinopsia (Choi et al., 2017) and visual hallucinations (Venkatesh et al., 2017) in patients on clomiphene — including male patients.
Visual symptoms that persist after stopping require ophthalmologic evaluation — do not wait to see if they resolve on their own.
Estrogen Elevation
Because LH rises and drives testosterone production, estradiol (E2) can rise in parallel — testosterone converts to estrogen via aromatase. Some men run high enough E2 to require an aromatase inhibitor adjunct. Regular lab monitoring of both T and E2 is standard practice.
Paradoxical Sperm Decline
Already covered above — but worth repeating: 19–24% of men on CC experience worsening semen parameters (Gundewar et al., 2021). Baseline and follow-up semen analysis is non-negotiable if fertility is the goal.
What Clomid Does NOT Appear to Do
Retrospective studies tracking PSA and hematocrit in men on CC have not found the same PSA elevation or hematocrit/polycythemia risk seen with TRT (Chandrapal et al., 2016). This is part of why it is sometimes preferred in men with borderline hematocrit or prostate concerns — though it does not mean zero monitoring.
ranked #1 for sperm concentration improvement across all treatment arms in a 2025 network meta-analysis — P-score 99% (Santi et al., 2025)
Dosing: What Studies Have Used
Clomid has no FDA-approved dosing protocol for men, so what physicians use is derived from the clinical literature. Commonly studied dosing regimens include:
- 25 mg every other day — the dose that ranked highest for sperm concentration improvement in the 2025 network meta-analysis (Santi et al., 2025)
- 25–50 mg daily — the range used in most retrospective safety studies
- 50 mg daily or every other day — used in the RCT showing T rising from 371 to 806 ng/dL (Shukla et al., 2025)
The general principle is to use the lowest effective dose. Higher doses do not reliably produce proportionally better testosterone responses — at higher doses, estrogen tends to rise disproportionately as aromatase converts the excess testosterone, which is why dose titration and regular E2 monitoring are standard practice.
Dosing is titrated based on labs — T, LH, FSH, and E2 levels — not on symptoms alone. This is not something to self-experiment with.
Frequently Asked Questions
Can I take Clomid instead of testosterone to keep my fertility?
Yes, and this is exactly the clinical scenario it is most commonly used for. Clomid raises testosterone through the hypothalamus-pituitary-testes axis rather than replacing it externally — which means LH, FSH, and sperm production are preserved or even increased. It is one of the primary options for men with secondary hypogonadism who want to maintain fertility while addressing low T symptoms.
How much does Clomid raise testosterone in men?
In clinical studies, average testosterone increases range from roughly 150 to 275 ng/dL across population averages. Individual responses vary significantly. In a recent RCT, men starting at a mean of 372 ng/dL reached over 800 ng/dL on 50 mg daily (Shukla et al., 2025). Some men respond more modestly. Response depends on how intact the HPG axis is and baseline LH/FSH levels.
What is the difference between Clomid and enclomiphene?
Clomid is a racemic mixture containing both enclomiphene (~62%) and zuclomiphene (~38%). Enclomiphene is the active anti-estrogenic isomer that drives the T increase. Zuclomiphene has weak estrogenic activity and accumulates with long-term use. Enclomiphene (Androxal) is the purified version — no zuclomiphene, potentially fewer side effects. The enclomiphene article covers the specific trial data comparing them.
Does Clomid for men work long-term or does it stop working?
The long-term data is limited, but existing follow-up studies of up to several years show maintained testosterone levels without significant tachyphylaxis (loss of response). The zuclomiphene accumulation issue (see above) is a theoretical concern for very long-term users. Most clinical protocols use Clomid until fertility goals are achieved or until the patient transitions to another approach.
Will Clomid cause vision problems in men?
Visual disturbances are a documented side effect — blurred vision, trailing images (palinopsia), and scotomata have all been reported in both male and female users (Viola et al., 2011). They occur in a minority of users but are the one side effect that warrants immediate cessation if it appears. Any change in vision while on Clomid should be evaluated same-day.
Is Clomid Right for You?
Clomid for men isn't a universal substitute for TRT, and it's not the right choice for every man with low testosterone. If the issue is primary testicular failure, it won't work. If maximum, predictable testosterone levels are the priority, TRT typically delivers better numbers.
But for a specific patient — a man with secondary hypogonadism, intact testes, and a desire to preserve or improve fertility — Clomid is a legitimate, evidence-backed option. The mechanism is sound, the efficacy data is consistent, and the safety profile (outside of the visual side effect and the paradoxical sperm decline risk) is generally favorable.
The off-label status means there's no standardized protocol handed to physicians. Treatment needs to be individualized — based on labs, goals, and follow-up monitoring — not pulled from a generic guide.
If this is a path you want to explore, HEXIS starts with a complete hormone panel, not a protocol handed to everyone who walks in the door. Book a consultation to go over your numbers with a provider who understands where Clomid fits and when a different approach makes more sense. Schedule a consultation
Clomid for Men: The Bottom Line
- 1
Clomid (clomiphene citrate) raises testosterone by blocking hypothalamic estrogen receptors — stimulating your own testes rather than replacing testosterone externally. Mean increases of +273 ng/dL in SR/MA data; individual RCTs show men doubling their T levels.
- 2
The defining advantage over TRT is fertility preservation: LH, FSH, and sperm production stay active. But 19–24% of men show paradoxical sperm decline on CC, and 17% don't recover — semen monitoring is non-negotiable.
- 3
Clomid is entirely off-label for men. It works for secondary (hypogonadotropic) hypogonadism where the testes are functional but under-signaled. It will not work for primary testicular failure. Treatment requires individualized dosing, lab monitoring, and a physician who knows the difference.