HCG for Men: Fertility & TRT — The LH Analog Explained
HCG for Men: Fertility & TRT — The LH Analog Explained
Most men who start testosterone replacement therapy don't realize they're shutting off a signal their testicles need to work. hCG for men solves that problem by directly replacing that signal — not by tweaking hormones upstream, but by talking to the Leydig cells themselves. Here's what it actually does, what the numbers show, and why a normal blood test doesn't tell you the whole story.
The short answer: hCG mimics LH (luteinizing hormone) and directly stimulates the testicles to produce testosterone from inside. On TRT, the body stops making LH — which cuts intratesticular testosterone by about 94%. Adding low-dose hCG reverses that suppression and keeps the testicles producing the testosterone sperm production actually depends on.
What Is hCG and How Does It Work in Men?
hCG is not testosterone. Human chorionic gonadotropin is a gonadotropin — a hormone in the same family as LH and FSH, the two signals your pituitary normally sends to your testicles.
When hCG enters your bloodstream, it binds to the same LH receptor on Leydig cells that your natural LH does. The Leydig cells can't tell the difference. They respond by producing testosterone — specifically, the testosterone inside the testicle itself, called intratesticular testosterone (ITT).
Here's the number most people don't know. Your serum testosterone — the value on your blood test — is only about 1.2% of what's actually inside your testicles (Coviello et al., 2005). The testicles maintain a concentration of testosterone roughly 80 times higher than your bloodstream. That concentrated environment is what spermatogenesis requires. A normal blood test tells you nothing about whether that environment is intact.
hCG's job is to keep that environment intact. Unlike the SERM-based approaches used in clomiphene therapy for men or enclomiphene, hCG bypasses the hypothalamus and pituitary entirely. It acts directly at the end organ — the testicle — which makes it effective even when the entire pituitary axis is suppressed.
94.0% relative scale
drop in intratesticular testosterone when men take TRT without hCG — from 1,174 nmol/L down to 72 nmol/L within three weeks (Coviello et al., 2005)
What TRT Does to Intratesticular Testosterone
TRT suppresses intratesticular testosterone by 94% — and a normal blood test will never show it.
When you take exogenous testosterone — injections, gels, or pellets — your brain reads elevated blood levels and tells the pituitary to stop sending LH and FSH. This is the HPG axis doing exactly what it's supposed to do. The unintended side effect is that your testicles go quiet.
In a controlled trial of 29 healthy men given testosterone enanthate plus saline placebo, LH dropped to 5% of baseline and FSH dropped to 3% of baseline within three weeks (Coviello et al., 2005). The effect on intratesticular testosterone was even more dramatic: ITT fell from a baseline of 1,174 nmol/L to 72 nmol/L — a 94% reduction.
That's the number behind the fertility concerns with TRT. Serum testosterone looks great on the blood test. Intratesticular testosterone — the number sperm production actually depends on — has essentially collapsed. An estimated 3 million American men were on testosterone therapy as of 2015 (Wenker et al., 2015), the majority likely unaware this was happening in their testicles.
Across different TRT formulations, the degree of ITT suppression varies. Research comparing nasal, intramuscular, and subcutaneous pellet testosterone found that intramuscular testosterone cypionate reduced 17-hydroxyprogesterone (an ITT surrogate marker) by 65.3%, while intranasal testosterone reduced it by only 33.3% (Diaz et al., 2023). No formulation fully preserves ITT without additional intervention.
hCG directly addresses this. By mimicking LH at the Leydig cell level, it keeps ITT from crashing even while the pituitary axis is suppressed by exogenous testosterone.
hCG Dose vs. Intratesticular Testosterone
Men on testosterone enanthate 200 mg/week — ITT change from baseline after adding hCG every other day (Coviello et al., 2005; n=29)
| hCG Dose | ITT vs. Baseline | Clinical Meaning |
|---|---|---|
| No hCG (TRT alone) | −94% | Essentially collapsed |
| 125 IU EOD | −25% | Still substantially suppressed |
| 250 IU EOD | −7% | Near-normal — preferred co-therapy dose |
| 500 IU EOD | +26% | Above baseline — fertility protocol range |
Source: Coviello et al., J Clin Endocrinol Metab, 2005 (PMID 15713727)
The Dose-Response: How Much hCG Is Needed?
The minimum effective co-therapy dose is 250 IU every other day — enough to hold intratesticular testosterone within 7% of normal.
The 2005 Coviello study mapped out exactly how much hCG is needed to counteract TRT-induced ITT suppression. The 29 men in the study received one of three hCG doses alongside testosterone enanthate, every other day:
- 125 IU EOD: ITT remained 25% below baseline — still substantially suppressed
- 250 IU EOD: ITT was only 7% below baseline — near normal
- 500 IU EOD: ITT was 26% above baseline — slightly above normal
This dose-response curve is the clinical foundation for the 250–500 IU EOD range most specialists now use for TRT co-therapy (Coviello et al., 2005). The 250 IU dose holds ITT at near-normal levels. The 500 IU dose pushes it above baseline, which can be useful when the goal is active fertility preservation.
For standalone treatment of secondary hypogonadism, dosing is higher. In a study of men with hypogonadotropic hypogonadism (HH) who had completed infertility treatment, hCG dosing ranged from 2,000–7,500 IU per week (Shiraishi et al., 2021). At these doses, hCG functions as a full LH-replacement signal, raising serum testosterone while preserving the testicles' structural integrity.
Higher doses come with a tradeoff. Leydig cells produce estradiol via aromatase activity, and more hCG stimulation drives more aromatization. At higher doses, estradiol elevation is common — which is why some men on hCG-based protocols also use a low-dose aromatase inhibitor to manage estrogen.
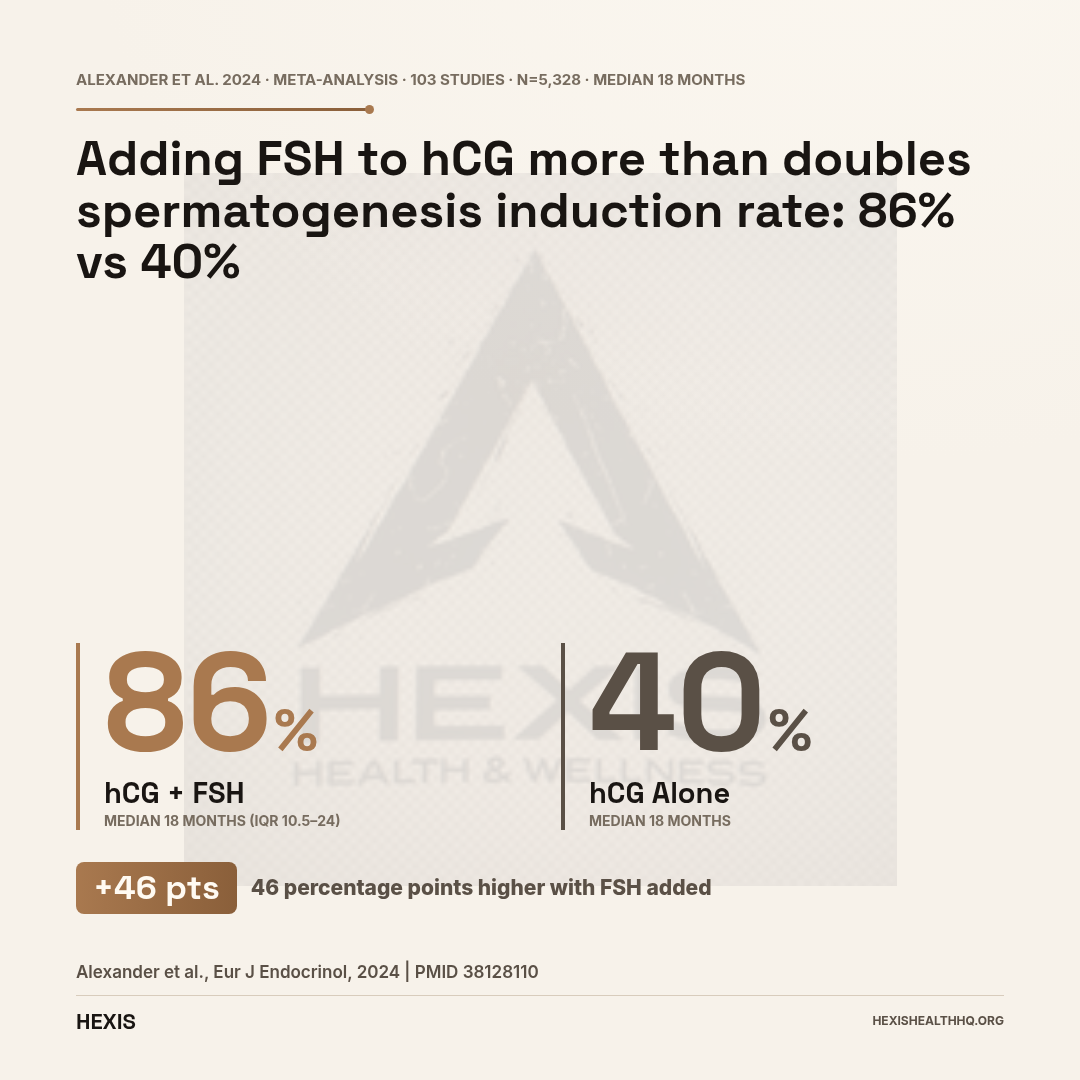
86.0% relative scale
spermatogenesis induction rate with hCG + FSH combined — versus 40% with hCG alone — across 5,328 patients and 103 studies (Alexander et al., 2024)
hCG for Spermatogenesis: When Fertility Is the Goal
hCG alone achieves spermatogenesis in only about 40% of cases — adding FSH pushes that rate to 86%.
The context matters: after TRT has suppressed spermatogenesis, or in men with hypogonadotropic hypogonadism who have never had normal sperm production, hCG alone is rarely sufficient.
A systematic review and meta-analysis across 5,328 patients and 103 studies found that hCG combined with FSH achieved a spermatogenesis induction rate of 86% (95% CI: 82–91%), compared to only 40% (95% CI: 25–56%) with hCG alone (Alexander et al., 2024). That gap exists because FSH drives Sertoli cell activity — and Sertoli cells are what actually support sperm maturation. hCG can restart testosterone production in the testicle, but without FSH signaling, sperm production often remains incomplete.
That's why the hCG + FSH combination is standard for hypogonadotropic hypogonadism when a man actually wants to father children.
The timeline is also longer than most men expect. A meta-analysis of 1,673 patients treated with gonadotropins found an average sperm concentration of 11.6 million per mL (95% CI: 8.4–14.9 M/mL) — with a median treatment duration of 18 months (Muir et al., 2025). By the end of treatment: 78% of men had any measurable sperm, 55% reached 1 million/mL, and 15% reached the WHO normal threshold of 20 million/mL.
That 18-month number is the one most men don't hear upfront.
How Quickly Does Spermatogenesis Come Back?
With hCG-based gonadotropin therapy, median time to measurable sperm is 18 months — and some men take longer. Set that expectation early.
The timeline also varies by approach, not just whether hCG is in the protocol.
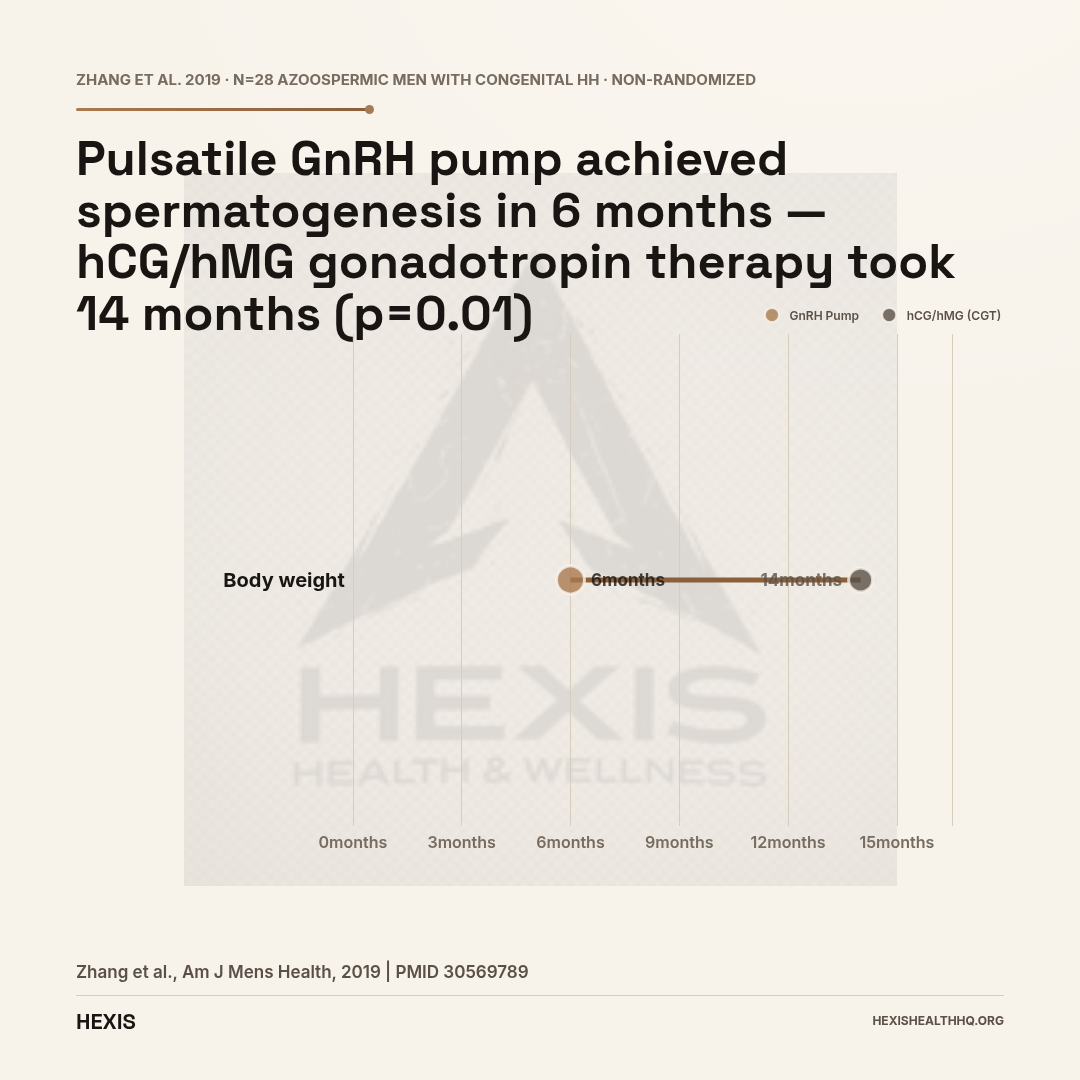
In a study of 28 azoospermic men with congenital hypogonadotropic hypogonadism, pulsatile GnRH pump therapy achieved spermatogenesis in a median of 6 months, while cyclical gonadotropin therapy using hCG and human menopausal gonadotropin took a median of 14 months (p = .01) (Zhang et al., 2019). By 24 months, both approaches reached similar success rates — the pulsatile pump was just faster.
The GnRH pump more precisely replicates the body's natural signaling and is faster when available. The hCG-based approach is the standard in most clinical settings because GnRH pump therapy is more technically demanding and less widely accessible.
For men recovering from TRT-induced suppression — rather than treating primary HH — recovery timelines are generally shorter, since the axis was previously functional. But expectations should still be set at months, not weeks. Sperm banking before starting TRT remains the cleanest option if future fertility is a near-term priority.
Wenker et al. (2015) published specific data on men who sought to recover spermatogenesis after testosterone use, finding that hCG-based combination therapy was effective for restoration in men who had been on TRT. The study noted roughly 3 million American men were on testosterone therapy at the time of publication — a figure that underscores why the fertility question matters at population scale.
hCG vs. Clomiphene and Enclomiphene: Why the Mechanism Matters
hCG works where SERMs cannot — directly at the Leydig cell, bypassing a pituitary that's already been suppressed by exogenous testosterone.
hCG, clomiphene, and enclomiphene all appear on the same list of options for secondary hypogonadism. They all raise testosterone and can support spermatogenesis. Their mechanisms, though, are fundamentally different — and that difference determines when each one is the right tool.
Clomiphene and enclomiphene are SERMs — selective estrogen receptor modulators. They work upstream, blocking estrogen receptors at the hypothalamus and pituitary to reduce negative feedback and cause the pituitary to release more of its own LH and FSH. The entire HPG axis remains active. The testicles receive a real signal from the pituitary.
hCG bypasses all of that. It acts directly at the Leydig cell, regardless of what's happening upstream. This is why hCG is uniquely effective in men on TRT: the pituitary is suppressed by exogenous testosterone and won't respond well to SERM-induced estrogen-receptor blockade. hCG can still drive ITT even when LH is at 5% of baseline (Coviello et al., 2005).
For a man not on testosterone therapy who wants to raise T while preserving fertility, a SERM may be appropriate. For a man already on TRT who wants to protect fertility or maintain testicular function, hCG is the direct and reliable option.
hCG Raises Estradiol — Monitor E2 at Any Dose
Leydig cells produce estradiol through aromatase activity, and hCG stimulates both testosterone and estradiol production. At co-therapy doses (250–500 IU EOD), the effect is modest. At standalone treatment doses of 2,000–7,500 IU/week, estradiol can climb into symptomatic ranges — causing mood changes, water retention, and gynecomastia.
Regular estradiol testing is standard on any hCG protocol. Men using higher doses may need low-dose aromatase inhibitor support. Do not self-adjust dose without lab guidance.
Source: Shiraishi et al., Endocrine J, 2021 (PMID 33012744)
Side Effects and Monitoring on hCG
hCG is well-tolerated at the doses used in clinical practice. Side effects map directly to what it does — stimulate Leydig cells — so the pattern is predictable.
Estradiol elevation is the most common concern. Leydig cells produce both testosterone and estradiol, so stimulating them with hCG raises both. At higher doses — especially the 2,000+ IU/week range used for standalone therapy — estradiol can climb into ranges that cause symptoms: mood changes, water retention, and gynecomastia (breast tissue development or tenderness). Estradiol monitoring and possible aromatase inhibitor support are standard in higher-dose protocols.
Injection site reactions are typical for subcutaneous injections. Most patients prefer the sub-Q route over intramuscular. Testicular discomfort or fullness at higher doses is occasionally reported, particularly early in treatment. Acne flares, driven by increased androgen activity, are also possible.
Leydig cell desensitization is a theoretical concern at chronically elevated doses. The LH receptor can downregulate with excessive stimulation — one reason low-dose co-therapy protocols (250–500 IU EOD) have replaced the older high-dose regimens in current clinical practice.
Monitoring on hCG should include serum testosterone, estradiol, and FSH/LH at regular intervals. If fertility is the goal, a semen analysis at 3–6 months tells you more than any hormone panel will — it's the direct read on whether spermatogenesis has actually restarted.
Is Compounded hCG Still Available?
Compounded hCG for men was effectively eliminated as a low-cost option in 2020, when the FDA removed it from the list of bulk substances eligible for 503A pharmacy compounding. Brand-name products — Pregnyl and Novarel — remain FDA-approved and available, but at higher cost.
Some providers shifted to alternatives — enclomiphene, kisspeptin agonists — for cost-driven reasons after 2020. Cost and access are real issues that matter upfront — ask your provider specifically about brand-name hCG pricing before assuming it fits your budget.
Frequently Asked Questions
Can I use hCG to maintain fertility while on TRT?
Yes — this is the most common use. Adding hCG, typically 250–500 IU every other day, keeps intratesticular testosterone near-normal even when the pituitary axis is fully suppressed. At 250 IU EOD, ITT stays within 7% of baseline, versus the 94% drop seen with TRT alone (Coviello et al., 2005). It does not guarantee fertility, but it preserves the testicular environment sperm production requires.
What is the standard hCG dose for men on testosterone?
For co-therapy alongside TRT, the most evidence-supported range is 250–500 IU every other day — the dose range that keeps intratesticular testosterone near baseline (Coviello et al., 2005). For standalone secondary hypogonadism treatment, dosing typically runs 2,000–7,500 IU per week, titrated to serum testosterone response (Shiraishi et al., 2021). Dosing should always be individualized based on labs and goals.
How does hCG differ from TRT for treating low testosterone?
TRT delivers exogenous testosterone, which shuts down LH and FSH — serum T rises but the testicles go quiet and may atrophy. hCG mimics LH directly at the Leydig cell, stimulating the testicles to produce their own testosterone while maintaining their function and size. Research in hypogonadotropic hypogonadism patients found that hCG-based treatment preserved testicular integrity in ways that conventional TRT did not (Shiraishi et al., 2021). The tradeoff: more frequent injections.
Does hCG raise estrogen levels?
Yes, it can. Leydig cells produce estradiol as well as testosterone, so hCG stimulation drives both. Estradiol elevation is a real possibility — particularly at doses above 500 IU EOD for co-therapy, or at standalone doses of 2,000+ IU/week. This is why estradiol monitoring is standard in responsible hCG management, and why some protocols include low-dose aromatase inhibitor support if E2 climbs into symptomatic territory.
How quickly do sperm return after using hCG post-TRT?
Recovery timelines are longer than most men expect. In a meta-analysis of 1,673 patients on gonadotropin therapy, median time to measurable sperm was 18 months, with an average concentration of 11.6 million/mL achieved (Muir et al., 2025). Some men recover faster; others take longer. If fertility is a near-term priority, sperm banking before starting TRT is worth a serious upfront conversation.
Working with HEXIS on hCG Protocols
Getting hCG dosing right requires lab work, not guesswork. Your provider needs your baseline hormone panel, serum testosterone and estradiol response to titration, and a clear understanding of whether the goal is fertility preservation, fertility restoration, or simply maintaining testicular function alongside TRT.
At HEXIS, board-certified physicians oversee every protocol. Every case starts with a full hormone panel — not a one-size protocol. If hCG is part of the picture, whether as a co-therapy alongside testosterone or as standalone treatment for secondary hypogonadism, dosing is built around your actual numbers and monitored appropriately. Estradiol doesn't manage itself.
Schedule a consultation to review your labs and discuss whether hCG fits your goals.
HCG for Men: The Bottom Line
- 1
hCG is an LH analog that directly stimulates the testicles — bypassing a suppressed pituitary axis entirely. On TRT, adding 250 IU every other day keeps intratesticular testosterone within 7% of normal, preserving the environment spermatogenesis depends on.
- 2
For fertility restoration in hypogonadotropic hypogonadism, hCG alone is rarely enough — the hCG + FSH combination achieves an 86% spermatogenesis induction rate versus 40% with hCG alone. Expect 18 months of treatment to reach meaningful sperm concentrations.
- 3
Estradiol elevation is the primary side effect to watch. Higher doses drive more aromatization, so regular E2 monitoring and possible aromatase inhibitor support are standard parts of any well-managed hCG protocol.